This is an automatically translated article.
The article is written by Master, Doctor Mai Vien Phuong- Gastroenterologist - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.Gastrointestinal submucosal tumors are tumors that arise from the myo-mucosa, submucosa, or muscular layer of the gastrointestinal tract wall. The most common submucosal tumor is in the stomach with a frequency of 1/300 cases of gastroscopy. The disease is characterized by a circular lesion that protrudes into the lumen of the gastrointestinal tract covered by normal mucosa and is discovered incidentally during gastroscopy or routine colonoscopy.
There are many patients who are often afraid when the doctor diagnoses themselves with a submucosal tumor, not knowing whether this tumor is large or small, benign or malignant, how to treat it, whether taking medicine will go away, is it necessary? After treatment, will it recur elsewhere....? All questions and questions above will be introduced by the doctor in the following article:
1. What is a gastrointestinal submucosal tumor?
Gastrointestinal submucosal tumors are tumors that arise from the myo-mucosa, submucosa, or muscular layer of the gastrointestinal tract wall. The most common submucosal tumor is in the stomach with a frequency of 1/300 cases of gastroscopy. Submucosal tumors are characterized by a circular lesion protruding into the lumen of the gastrointestinal tract covered by normal mucosa and are incidentally detected during routine gastroscopy or colonoscopy.
Most submucosal tumors are small (< 2 cm) and asymptomatic, but submucosal tumors can cause hemorrhage, gastrointestinal obstruction, or metastasis depending on tumor size, location, and histological nature. Treatment of submucosal tumors mainly focuses on accurate diagnosis and determination of the risk of malignancy of the lesion. 85% of submucosal tumors are benign, the remaining 15% are malignant. Because submucosal tumors are located under the mucosa, conventional alkaline biopsy techniques will not determine the nature of the tumor, often requiring the use of new diagnostic and biopsy techniques such as endoscopic ultrasound and aspiration. with a fine needle through endoscopic ultrasound to confirm the diagnosis of submucosal tumors.
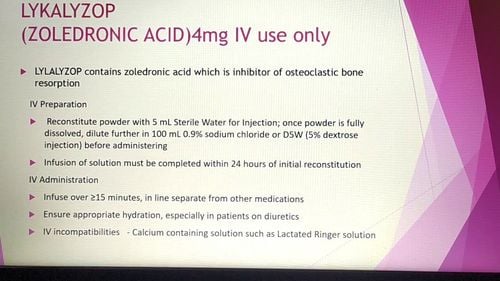
Hình 1: Cấu tạo thành ống tiêu hoá
2. Submucosal tumors are structures located under the mucosal layer
Endoscopic ultrasonography is the most accurate imaging method for the evaluation of gastrointestinal submucosal tumors because of its ability to individually delineate each layer of the gastrointestinal tract wall and precisely determine the location of the submucosal tumor. The layers of the gastrointestinal tract wall on the inside-out endoscopy are: mucosa and myo-mucosa, submucosa, muscle layer, and serosa.
Endoscopic ultrasound has higher accuracy than computed tomography and magnetic resonance imaging in the diagnosis of small submucosal tumors (< 2 cm). This imaging method can accurately distinguish tumors in the gastrointestinal tract wall from external tumors pressing on the gastrointestinal tract (30% of suspected cases of submucosal tumors are tumors from the outside pressing on the digestive tract). chemical). Endoscopic ultrasound can measure the size of the submucosal tumor and evaluate the surrounding lymph nodes. Finally, endoscopic ultrasound fine-needle aspiration or endoscopic ultrasound biopsy helps to determine the histological nature of the submucosal tumor and prescribe appropriate treatment.
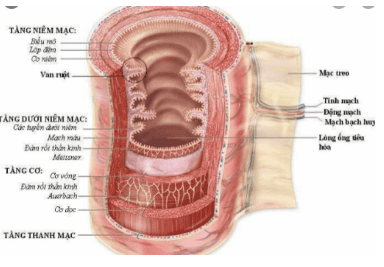
Hình 2: Siêu âm nội soi đánh giá u dưới niêm thực quản

Hình 3: Đầu dò siêu âm được tích hợp ở đầu ống soi tiêu hóa
3. Types of tumors under the lining of the gastrointestinal tract
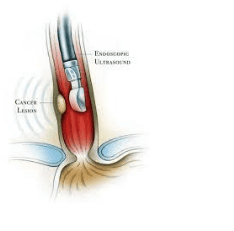
Gastrointestinal stromal tumor is the most common mesenchymal tumor of the gastrointestinal tract. This tumor is of Cajal cell origin and can occur at any site of the gastrointestinal tract. GIST is most commonly found in the stomach (60 - 70%), followed by the small intestine (20 - 30%), colon (5%) and esophagus (5%). Tumors are usually spherical or rhomboid, and usually originate in the muscularis or mucosal layer. GISTs should be classified according to the likelihood of malignancy based on tumor location, tumor size, symptom onset, and histopathologically mitotic count. GISTs in the small intestine are more likely to be malignant than GISTs in the stomach. Surgery is usually indicated for symptomatic GIST tumors (pain, obstruction, bleeding), regional lymphadenopathy, size > 2 cm, and small bowel GIST. GIST < 2 cm with high risk factors on endoscopic ultrasound (irregular boundaries, internal cysts, ulcers, heterogeneous echoes) also require surgical treatment. Low-risk cases of GIST < 2 cm should be followed up with endoscopic ultrasound every 6 to 12 months.
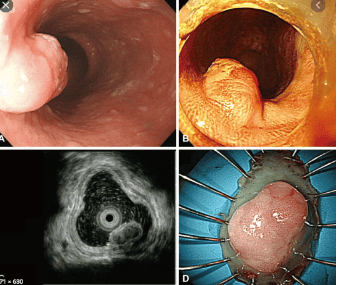
Hình 4: Hình ảnh u GIST – U trung mô đường tiêu hóa ở phình vị trên nội soi và nội soi siêu âm
3.1. Smooth muscle tumor
Gastrointestinal smooth muscle tumor is a benign muscle tumor arising from the muscularis or mucosal layer. Most leiomyomas occur in the esophagus, rarely elsewhere in the gastrointestinal tract. 90% of esophageal leiomyomas are found in the middle and lower thirds of the esophagus. Surgical removal of the tumor is performed only when the tumor causes symptoms such as difficulty swallowing, bleeding, intestinal obstruction or perforation. SANS is a highly accurate method in diagnosing gastrointestinal stromal leiomyomas and distinguishing it from other types of UC, leiomyomas are usually located in the 4th layer, sometimes in the 2nd layer (mucosa). are structures with clear edges, uniform sound reduction. On the wall of the gastrointestinal tract, it is found mainly in the esophagus, less often in the stomach and duodenum, and sometimes in the rest of the body. Usually, leiomyomas are discovered incidentally, some have complications such as causing gastrointestinal obstruction (eg, causing difficulty swallowing when lying in the esophagus), gastrointestinal bleeding when ulceration... Pure leiomyomas are usually benign, especially connective leiomyomas tend to be malignant, on SANS are often less homogeneous, large in size (usually > 6cm), on histopathology with high mitotic index.
3.2. Fat tumor
Lipomas are common submucosal tumors and can be found in all locations of the gastrointestinal tract, most commonly in the colon and antrum. Lipomas are caused by an accumulation of adipose tissue, which is usually yellow on endoscopic images and feels soft to the touch with biopsy forceps. Lipoma biopsies are not necessary when the endoscopic appearance is typical. Lipomas usually do not cause symptoms, but large tumors can cause bleeding or intestinal obstruction, requiring surgery to remove the tumor. Lipomas do not pose a risk of malignancy, so surgery or follow-up is not necessary if the tumor is asymptomatic.
3. 3. Neuro-endocrine tumors
Neuroendocrine tumors of the gastrointestinal tract are also considered malignancies and are common in the small intestine. Some neuroendocrine tumors can secrete hormones and cause clinical syndromes. However, most of these tumors are discovered incidentally in the rectum, stomach, duodenum, or small intestine during endoscopy. Neuroendocrine tumors often originate in the muscle layer and invade the submucosa, so they can be diagnosed and biopsied using conventional endoscopic techniques. These tumors can be treated with endoscopic or surgical resection techniques, depending on the size, location, and differentiation of the tumor.
3.4. Ectopic pancreatic tissue
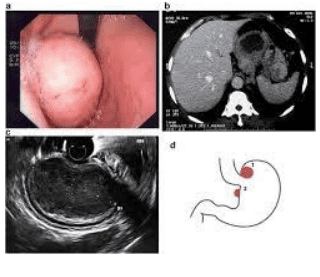
Ectopic pancreatic tissue is often discovered incidentally through gastroscopy, this lesion is usually in the antrum on the greater curvature of the stomach. Ectopic pancreatic tissue is a round-shaped submucosal tumor, covered with normal mucosa, with a central depression. This lesion is usually asymptomatic but can sometimes cause bleeding, abdominal pain, or bowel obstruction. Ectopic pancreatic tissue > 3 cm can cause acute or chronic pancreatitis.
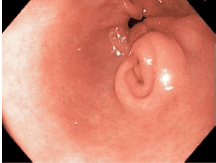
Hình 5: Hình ảnh mô tụy lạc chỗ ở hang vị
3.5. Double cyst
Double cysts are congenital abnormalities that occur during embryonic development and often attach to the wall of the gastrointestinal tract or penetrate into the lumen of the gastrointestinal tract. The cyst is lined by the lining of the gastrointestinal tract that contains mucus-secreting glands and causes the cyst to enlarge. Double cysts usually cause no symptoms but can cause difficulty swallowing, pain, or bleeding depending on the location of the cyst.
4. Diagnosis and treatment of gastrointestinal submucosal tumors
Submucosal tumors such as lipomas, double cysts, and ectopic pancreatic tissue can be diagnosed based on endoscopic imaging and do not require biopsy. However, other types of tumors such as GIST, leiomyoma, and other potentially malignant tumors require biopsy or resection to diagnose and confirm the possibility of malignancy. Submucosal tumors are often located deep below the mucosa, originating from the submucosa or muscle layer, so tissue biopsy is relatively difficult. Many techniques are used for diagnosis such as standard biopsy, large forceps biopsy, partial resection of tumor, excavated biopsy, fine-needle aspiration or endoscopic ultrasound needle biopsy, mucosal resection. through endoscopic or submucosal surgery through endoscopic, surgical...
5. The role of SANS in the treatment guidelines for gastrointestinal mucositis
Currently, people have attached to the end of the endoscope an ultrasound probe that allows to conduct ultrasound examination from within the gastrointestinal tract and this technique is called endoscopic ultrasound. This is a technique combining endoscopy and ultrasound, in which the ultrasound probe is approached closest (no longer the limitations of conventional ultrasound such as gas, image noise...) to the lesions to be examined. endoscopic probe: damage to the wall of the esophagus, stomach, intestines, liver, pancreas and biliary tract.
In cases of GIST with symptoms, large size and/or features suggestive of malignancy on SANS, resection of the tumor is the most effective treatment. In contrast, GISTs that are small, asymptomatic, and consistent with benign imaging require only follow-up. But in clinical practice, it is often difficult to advise on how to treat patients when the nature of GIST cannot be determined through SANS, it is necessary to consider many factors and depending on the specific case.
Esophageal GIST is usually benign and, if asymptomatic, should be monitored. Gastric GIST with indications for surgery can be done through laparoscopy, combined with oral endoscopy if necessary. Duodenal GIST surgery is often traumatic and invasive for patients, so it is only indicated for cases with high risk of malignancy. Colorectal GIST is uncommon and can be resected rectally in the lower rectum
Lipomas usually require only follow-up, but when they cause symptoms such as obstruction or bleeding, endoscopic resection and SANS can help. Avoid blood vessels, adjacent structures.
SANS also helps guide the treatment of gastrointestinal carcinoid by accurately measuring the size and pinpointing the location and extent of invasion within the layers of the gastrointestinal wall.
5.1. Endoscopic mucosal resection
Endoscopic mucosal resection is used to cut mucosal and submucosal tumors up to 2 cm in diameter. Mucosectomy can not only remove submucosal tumors, but also has high diagnostic value. However, when using this technique, caution should be exercised when resecting tumors originating from the muscle layer because of risks such as perforation, bleeding, or residual tumor. Therefore, this technique should only be used in the diagnosis and treatment of submucosal tumors arising from the muscularis or submucosa, and should not be used for submucosal tumors originating from the muscular layer or in the duodenum. .
5.2. Endoscopic submucosal dissection
Endoscopic submucosal resection can be used to diagnose and treat submucosal tumors. This technique can be performed for tumors originating in the muscularis or malignant submucosa. Submucosal resection can cut submucosal tumors larger than 2cm, but this is a difficult technique, takes a long time and has a high risk of complications when the tumor is over 5cm.
Hình 6: Kỹ thuật ESD cắt bỏ u dưới niêm ở thực quản
5.3. Endoscopic resection of the tumor through the submucosal tunnel
The first submucosal tunneling technique was used in the esophagus to cut the lower esophageal sphincter to treat achalasia. This technique was then used to cut submucosal tumors arising from the muscular layer of the esophagus and cardia. This technique includes steps: Make a mucosal incision at least 5cm away from the lesion, then the bronchoscope is inserted into the submucosa and gradually to the submucosal tumor, then the submucosal tumor is cut by the technique. submucosal resection (ESD) and finally closure of the mucosal incision after complete resection of the tumor.
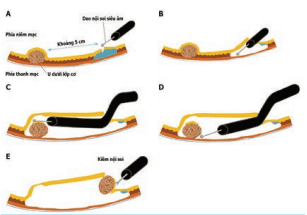
Hình 7: Cắt bỏ u nội soi qua đường hầm dưới niêm mạc
5.4. Endoscopic full-thickness resection of the gastrointestinal tract
Full-thickness gastrointestinal resection technique can perform and ensure complete tumor removal. Full-thickness gastrointestinal resection can be performed completely endoscopically. This technique can be performed with submucosal tumors up to 4 cm in size and in difficult locations such as gastric aneurysm or the upper part of the body. Conventional endoscopic resection techniques such as endoscopic mucosal resection or endoscopic submucosal dissection are powerful tools in the treatment of gastrointestinal neoplasms. However, these techniques are limited to the superficial layers of the gastrointestinal tract wall. However, there are cases where, for example, submucosal tumors arising from the muscle layer or invading the muscle layer, especially GIST tumors, need to be removed. At that time, it is possible to use the technique of endoscopic full-thickness resection of the gastrointestinal tract wall with the closure of the perforation in the gastrointestinal tract wall by specialized tools or in combination with laparoscopic surgery. This technique is now gradually becoming routine in clinical practice, it is not only a powerful tool for histological diagnosis but also potentially for surgical treatment in selected cases. However, in Vietnam, this technique has not been widely deployed, because it requires investment in equipment, and the skill of the endoscopist must also be thoroughly trained.
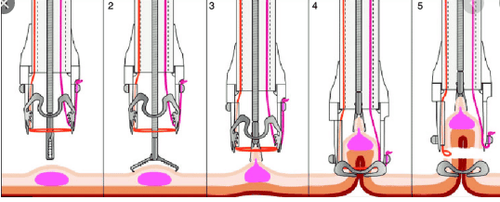
Hình 8: Hình minh hoạ kỹ thuật cắt toàn bộ thành ống tiêu hoá

Hình 9: Kỹ thuật cắt toàn bộ thành ống tiêu hoá điều trị u dưới niêm dạ dày
Tumor resection, atypical gastrectomy or resection of the gastrointestinal tract containing the tumor is used when endoscopic techniques fail due to large tumor, difficult location, tumor at risk of malignancy and have lymph node metastasis.

Hình 10: Phẫu thuật cắt u dưới niêm
Tumor under the gastrointestinal tract is not a rare disease, determining the nature of the tumor is very important, but it is limited when only endoscopic and common biopsies are available. essential in the diagnosis and treatment of this disease. Many submucosal tumors are benign and only need monitoring, but there are also many cases of complications. Fine-needle aspiration under endoscopic ultrasound guidance helps to determine the nature of the submucosal tumors. Information from endoscopic ultrasound results can help us to have the right attitude to manage submucosal tumors.
5. Advice for patients diagnosed with gastrointestinal submucosal tumors
GIST tumors in the stomach and colon are larger than 2 cm and are at high risk requiring surgical treatment. Endoscopic ultrasound should be used to diagnose and monitor submucosal tumors (especially submucosal tumors < 2 cm). Asymptomatic leiomyomas do not need to be monitored and treated endoscopically, avoiding waste of time, treatment costs, and risks of diagnostic procedures. Lipomas do not require endoscopic monitoring and treatment unless symptomatic. Submucosal tumors arising from the muscle layer need to be biopsied by fine needle aspiration to determine the nature of the lesion and have an appropriate treatment. (FNA) Submucosal tumors have the risk of malignancy and need to be removed endoscopically or surgically depending on the nature, size and location of the tumor, Vinmec International General Hospital is a prestigious address for many patients. reliable in performing endoscopic and endoscopic ultrasound for diagnosis of gastrointestinal submucosal diseases.... Especially, Vinmec is now equipped with modern facilities and equipment with the team. With a team of experienced experts, always dedicated to medical examination and treatment, customers can be assured of gastroscopy, esophagoscopy and colonoscopy services at Vinmec International General Hospital.
Customers who are interested in the technique of diagnosis and treatment of submucosal tumors at Vinmec need advice and support, please contact to register for an online examination.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.