This is an automatically translated article.
The article is written by Dr Department of Gastroenterology - Endoscopy, Vinmec Central Park International General Hospital.
95% of colorectal cancers arise from adenomatous polyps on the lining of the digestive tract. Therefore, removal of all polyps found during colonoscopy is the most effective screening method for colorectal cancer.
1. Why is colon cancer the first type of cancer to screen for?
According to screening standards, colon cancer is the type of cancer that should be screened first for the following reasons:
Common disease, accounting for 10% of all cancers. In Vietnam, it is the third and fourth leading cancer in which 6% of the population over 50 years old has colorectal cancer, which is the third leading cause of death. The trend in the frequency of the disease is increasing markedly. Progression is slow, from normal mucosa to benign adenoma, to cancer over a long period of 5 to 15 years. The cure rate after surgery is very high, over 90%. If the disease is detected at the precancerous stage of polyps, only endoscopic polypectomy or for early cancerous lesions that have not invaded the submucosa, Endoscopic mucosal surgery can be used. resection (EMR) or Endoscopic submucosal dissection (ESD), are minimally invasive techniques that treat colorectal cancer.

2. Types of screening tests
However, which test to use for screening is still controversial. The choice of screening method also depends on the health status, the level of risk of the subject and the facilities available at the medical facility.
The simplest is Fecal ocult blood testing (FOBT). The second test is iliacoscopy or total colonoscopy every 5 years or double-contrast colonoscopy.
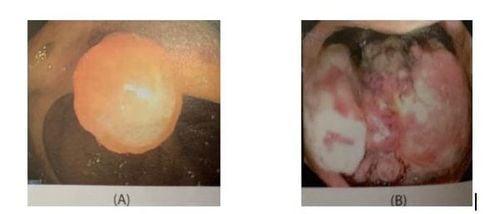
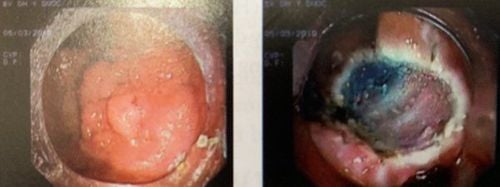
Stool blood test: shows 10% of patients with cancer or 34% of pre-existing polyps have changed but 50% of this test is negative when the patient has cancer. When the test is positive, the next step is to have a colonoscopy. It is recommended that people over the age of 50 annually check for blood in their stools to reduce cancer deaths by one-third. Pelvic colonoscopy: Also noted by the authors. In theory, pelvic endoscopy is more beneficial than fecal occult blood testing because of the greater chance of finding early damage. Furthermore, according to the literature, over 50% of colorectal cancers are found in the anorectal and pelvic colon. However, this method is disadvantageous because it can miss cancer located at a higher location, as well as the rate of 3-5% of cancers appearing in more than 2 places in the colon. Colonoscopy: Many authors agree on the recommendation to replace pelvic endoscopy with colonoscopy to adequately screen the entire colon. Colonoscopy is the only technique that can directly visualize the colonic mucosa, with magnification from 100 to 1,000 times greater than normal (Figure 4). Today, endoscopists can see changes at the histological level, instantaneously, with ultra-magnified endoscopic systems. In particular, in addition to the ability to diagnose sensitively, endoscopy is also the only technique that can perform polypectomy, mucosal resection (Figure 5), submucosal resection (Figures 6, 7, 8) of polyps. large or early colorectal cancer, biopsy suspected lesions.
However, this is an invasive technique, with a high rate of complications and complications from drug bowel preparation, anesthesia and anesthesia and the technique of implementation. The rate of these complications and complications also increased many times when comparing between diagnostic endoscopy and therapeutic endoscopy. Therefore, endoscopists need to be trained seriously, know the correct indications and know how to stop in time, which is the key to the success of an experienced endoscope.

Colonography: Should take a colonoscopy with contrast if the colonoscopy cannot cover the entire colon, because the patient cannot tolerate the colonoscopy or the medical facility is not qualified and has insufficient equipment. be completed. Dual-contrast contrast-enhanced colonoscopy is also more likely to show small lesions, precancerous polyps larger than 1cm in size. Contrast colonography also helps the surgeon to accurately locate the lesion on the colonic frame, which may be mistaken by the colonoscopy technique, especially when the colon is long and twisted. DNA testing: Today, medicine has identified the genes that cause disease. Therefore, comparing the DNA with the DNA of relatives who have had cancer before is the best way to screen for the disease, but it is expensive and not common.
3. Objects of screening
3.1 Screening for Lynch syndrome subjects, there are 02 groups. People with first-generation relatives (parents, brothers) have had colorectal cancer before the age of 45. These subjects are 10 times more likely to get cancer. times the average person, he has more than 2 first-generation relatives with any cancer. These subjects are 6 times more likely to get cancer than the general population. Because colorectal cancer often occurs from the age of 50, screening at this age can reduce the rate of cancer by 50% and prolong survival for more than 12 months. The test that should be used in these subjects is colonoscopy. If a very young family member, under 40 years of age, has cancer, family members should be screened 10 years earlier and colonoscopy should be performed every 5 years.
3.1.1 Hereditary non-polyposis colon cancer (HNPCC) This type of cancer (Figure 9) often runs in families and causes disease in young people, before the age of 45. In addition to colonoscopy. For family members every 5 years from the age of the person with the disease, a DNA test is needed to compare it with the DNA of a loved one who has had cancer before.
Subjects in this family need colonoscopy, gastroscopy, mammogram, pelvic ultrasound and cytology test because in addition to colon cancer they can have stomach cancer, cancer breast, uterus and ovaries.
Familial Adenomatous Polyposis (FAP) This disease is less common than non-polyposis colon cancer but will progress to colon cancer when over 50 years old, so all relatives should be screened. of patients who have had this disease starting at age 10, iliacoscopy or total colonoscopy. If FAP is present (Figure 10), a total colectomy should be considered to prevent malignant polyposis.

Follow-up after removal of malignant polyps: Colorectal polyps larger than 1cm, sessile, dysplasia have a high risk of malignant transformation. After endoscopic polypectomy, it is necessary to monitor and periodically check endoscopic examination as follows:
Every 01 month for the first 3 months, in the first year. Every 3 months for the next 6 months, in the first year. Every 6 months in the second year. Every year, from the 3rd to the 5th year. For malignant polyp lesions, the schedule for colonoscopy is similar to the follow-up schedule for colorectal cancers that have been operated on such as:
Blood tests for cancer markers letter (CEA) 06 months after surgery, for 05 years. Colonoscopy check 6 months after surgery, in the first year. Colonoscopy check 01 year after surgery, in the second year. Colonoscopy check 3 years after surgery, in the third year onwards. Monitoring inflammatory bowel diseases Inflammatory bowel diseases, including ulcerative colitis (Figure 11) and Crohn's disease, cause an inflammatory response in more than half of the colon and make patients 10 times more likely to develop cancer than the general population.
The authors recommend that if colitis is more than 8 years old, colonoscopy should be done annually. The primary goal is to detect precancerous lesions. If severe metaplasia is confirmed by at least 2 pathologists, total colectomy is recommended to prevent cancer.

4. Early colorectal cancer treatment
Removal of all polyps found during colonoscopy is the most effective screening for colorectal cancer. Gastrointestinal endoscopy can also intervene in the local treatment of these very early cancer lesions by endoscopic submucosal dissection (ESD) to help patients avoid a physically heavy surgery. as well as spiritual.



Gastrointestinal cancer screening at Vinmec International General Hospital is a scientific and effective measure to detect gastrointestinal cancer early and provide the best treatment regimen.
The package of screening and early detection of gastrointestinal cancer (esophagus - stomach - colon) of Vinmec hospital combines clinical and paraclinical examination to bring about the most accurate results possible. When registering for the package, customers will be instructed:
Gastroenterology examination with an Oncologist (by appointment) Gastroscopy and colonoscopy with NBI endoscope with anesthesia Laboratory total peripheral blood cell analysis (laser counter) Automated prothrombin time test Automated thrombin time test Activated Partial Thromboplastin Time (APTT) test by automatic machine General abdominal ultrasound If you need consultation and examination at Vinmec Hospitals of the national health system, please make an appointment on the website to be served.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.













