This is an automatically translated article.
The article was professionally consulted with Specialist Doctor I Le Thanh An - Interventionist Cardiologist - Department of Medical Examination & Internal Medicine - Vinmec Nha Trang International General Hospital.Angioplasty is a treatment method that is being widely applied thanks to its low invasive advantages, high success rate, especially for young children. As a result, patients avoid the risk of serious complications such as severe systemic hypertension, advanced coronary artery disease, stroke, aortic dissection, heart failure, and premature death.
1. Advantages of coarctation of the aorta
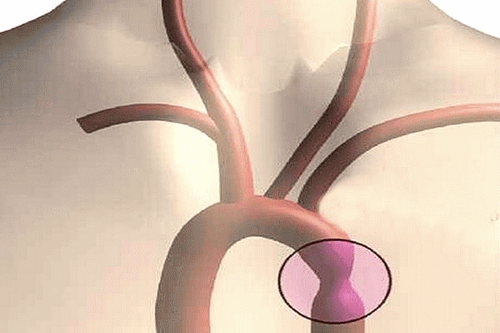
The aorta is the largest blood vessel, originating from the heart, branching into smaller arteries to carry blood and oxygen from the heart to all organs in the body. Coarctation of the aorta is a localized narrowing of the lumen of the thoracic aorta, just behind the bifurcation of the left subclavian artery. Patients with clinically significant coarctation of the aorta are at increased risk of developing long-term complications, including severe systemic hypertension, progressive coronary artery disease, stroke, aortic dissection, heart failure and premature death.Most cases of coarctation of the aorta are congenital; acquired causes are rarer.
Options to correct original discrete aortic coarctation (no prior intervention) include catheter intervention (eg, balloon angioplasty and/or stenting) and surgery. In the framework of this article, we only focus on the topic of balloon dilation and stenting.
Angioplasty - is an alternative to surgery for discrete coarctation of the aorta in neonates >4 months and infants weighing <25 kg. It is the preferred intervention for all patients with isolated coarctation of the aorta, regardless of age. However, stenting is an alternative to balloon angioplasty in older children (≥25 kg) and adults with original or long discrete coarctation of the aorta; In these patients, balloon angioplasty is an option if stenting is not feasible and surgery is not an option.
Stenting - In children and adults, stenting after balloon angioplasty or surgery maintains hemodynamic benefit by improving arterial diameter, thereby reducing pressure gradient across residual stenosis. Be minimized. Children who receive an aortic stent are more likely to need a planned second intervention than adults because the stent often needs to be enlarged as the child gets older. Stenting is generally not recommended in patients weighing <25 kg, because of possible femoral artery injury due to the need for a large sheath to insert the stent. In addition, the aorta in patients <25 kg is small. Although stents have been successfully placed in patients <30 kg, implantation of stents in these patients will require multiple interventions to expand the stent as they grow older. The risks associated with repetitive catheter interventions should be balanced against the more invasive risk of surgical repair. In clinical practice, we only consider stenting in patients who are large enough to receive a stent that can expand to adult size.
2. Indications and contraindications for coarctation of the aorta
Indications for coarctation of the aorta in the following cases: Waist difference at rest >20 mmHg: estimated based on difference in maximal blood pressure between upper and lower extremities or by color ultrasound. Alternatively, it is possible to measure directly through the catheter in the aortic dilatation (usually done during angioplasty or stenting of aortic coarctation); There is radiological evidence: there is significant collateral circulation; Systemic hypertension due to coarctation of the aorta; Heart failure due to coarctation of the aorta, most commonly seen in neonates with severe coarctation (however, may occur in older patients). Contraindicated for coarctation of the aorta when: The patient is suffering from other serious or acute diseases; The patient is allergic to contrast; Patients with hemostasis disorders; The patient refused to perform the procedure.
Hình ảnh mô phỏng tình trạng hẹp eo động mạch chủ
3. Cochlear aortic stenosis technique
3.1. Preparation before angioplasty Personnel: 2 doctors and 2 technicians specializing in interventional cardiology; Patient: Was thoroughly explained about the procedure, consented to the procedure and signed the consent form; intravenous prophylactic antibiotics; check kidney function and comorbidities; check for coagulopathy or allergy to contrast agents; sedation or endotracheal anesthesia (for young children), local anesthesia (for older children and adults); Medical records: Prepare according to regulations; Tools: Table for tools (including sterile bowls, gloves, surgical gowns, sterile dressings); Three-prong device, sterile gauze, pump capacity of 5ml - 10ml - 20ml; Angioplasty kit (includes 1 needle, 1 sheath and local anesthetic); Terumo 0.035 inch curved and straight end lead, MP catheter, pigtail catheter, stiff wire, coronary guidewire; Balloons of all sizes; Contrast and imaging pump; Aortic stents of all sizes; Emergency support facilities: Balloon, oxygen mask, endotracheal tube, electric shock machine, temporary pacemaker,... 3.2. Performing the technique of vascular access: The doctor disinfects the large skin around the patient's vascular access area, then opens the entrance (usually the right femoral artery). If the patient has a tight stenosis, the right radial line can be added (for adults) Heparin injection for the patient: Intravenous heparin is given to the patient at a dose of 70-100 units/kg body weight before administration. intervention tool. When the procedure is prolonged, the doctor should perform an activated clotting time test (target is 250 - 350 seconds). If the activated clotting time is low, an additional dose of Heparin is required. 1000 units of Heparin can be added 1 hour after the procedure; Aortic angiography identifies lesions: The doctor inserts a pigtail catheter with a wire terumo straight into it leading up to the aortic arch - above the narrowing site (it can be followed by the femoral artery or the right radial artery). Then, the doctor took an angiogram to determine the location and size of the lesion of the isthmus as well as the correlation of the location of the stenosis with the left subclavian artery; Angioplasty and stenting of the aorta: The physician drives the MP catheter from the right femoral artery with a terumo-guided wire through the isthmus to reach the superior aorta; After that, replace the terumo conductor with a super stiff conductor; Next, the doctor slides the hot balloon on the super stiff wire, dilating the location of the coarctation of the aorta by adjusting the pressure and increasing the balloon size. After each dilation, the doctor re-checks the pressure difference across the waist. The maximum size of the balloon will be based on the reference size of the aorta above and below the site of stenosis. If the narrowing is increased in size, there is no longer a pressure gradient across the waist that is a successful dilation. At this point, the doctor withdraws the balloon and leaves the guide wire; Immediately, the doctor put the stent on the wire to go to the site of the narrowing lesion and performed an examination. When the stent is in place, the doctor performs balloon dilation so that the stent expands, hugging the aortic wall. The time to inflate the balloon is about 10-15 seconds. If the stent has not fully expanded, it can be re-expanded. Then, measure the difference in pressure after stenting and check again. If there is no pressure gradient across the waist and the stent is well dilated, the procedure is successful; The doctor pulled out the catheter system, stitched to stop the bleeding for the puncture wound, and then applied pressure.
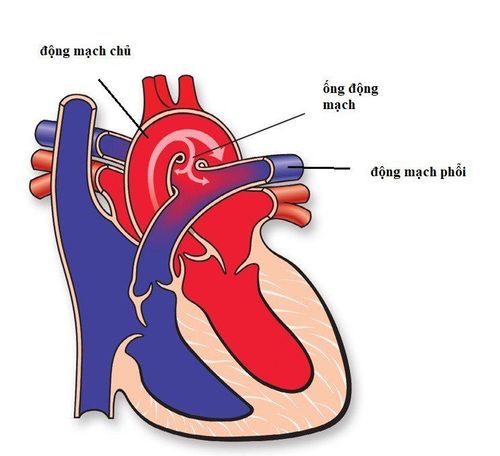
Hình ảnh trước và sau nong hẹp eo động mạch chủ
Pulse, blood pressure, monitor for signs of hypovolemic shock if present; Check the thigh area on the side of the puncture to promptly detect if there is bleeding or formation of a hematoma; Check the patient's blood pressure in both the upper and lower extremities. Instruct the patient on the following issues:
Stay in bed for the first 6 hours after angioplasty, keep the leg on the interventional side for the first 2 hours; When coughing or sneezing, keep the puncture site pressed. If you find recurrent bleeding or a lot of pain in the intervention area, you should immediately call a medical staff; Drink extra water to prevent the risk of low blood pressure and kidney disease caused by the use of contrast; Take the correct dose of aspirin for 6 months. 3.4. Risk of complications and interventions Aortic dissection: This complication can be prevented with adequate balloon pressure and the use of new generation stents. Management is pain relief, heart rate control, blood pressure, stent grafting or surgery; Loss, drop or displacement of instrument: Treat by contacting emergency surgery immediately; Embolism due to gas, blood clot formed on the surface of the instrument: It is necessary to prevent by correcting the procedure and using a full dose of Heparin, combined with taking Aspirin within 6 months after the intervention; Other complications: Complications of pain-induced vagal episode causing bradycardia, hypotension (manage by giving the patient atropine or vasopressors if needed), contrast agent allergy or anaphylaxis (need to detect Early detection and proper treatment of standard regimen), infection (rare - correct treatment), complications at the puncture site (managed according to standard protocol),... Angioplasty with balloon and stent is a technique with high success rate and high safety. When this procedure is indicated, the patient should cooperate well with the doctor to ensure the highest treatment effect and minimize the risk of unwanted complications.
To protect cardiovascular health in general and detect early signs of coarctation of the aorta, customers can go to Cardiovascular Center - Vinmec International General Hospital for appropriate examination and treatment. As one of the leading cardiovascular centers in the country in terms of examination, diagnosis, screening and treatment of cardiovascular diseases, Vinmec not only has the convergence of a team of experienced and leading experts. prestigious in the field of surgical, internal medicine, interventional cardiac catheterization but also has a system of modern equipment, on par with the most prestigious hospitals in the world such as: 3 Tesla MRI Magnetic Resonance Machine (Siemens), CT 640 (Toshiba), high end endoscopes EVIS EXERA III (Olympus Japan), high-end anesthesia system Avace, Hybrid operating room according to international standards... Especially, with The space is designed according to 5-star hotel standards, Vinmec ensures to bring patients the most comfort, friendliness and peace of mind.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.