This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General HospitalAmyloidosis is characterized by extracellular deposition of abnormal proteins, including primary, secondary, hemodialysis-associated, hereditary, and focal. Primary amyloidosis division involves monoclonal light chains. Secondary amyloidosis is associated with inflammatory diseases, infections, and cancer. Amyloid deposition in the gastrointestinal tract can manifest with symptoms including diarrhea, diarrhea, or constipation.
For diagnosis, one should obtain an immunostain of serum or urine as well as a biopsy of the gastrointestinal mucosa that is specifically stained. While most gastrointestinal complications are controlled with symptoms, treatment depends on the type of amyloidosis.
1. Latest perspectives on pathogenesis
Amyloidosis is defined as the extracellular deposition of protein filaments with β-filamentous structure and characteristic properties usually after staining with Congo Red dye. The current nomenclature consists of the first letter, A (for amyloid), followed by a description of the precursor protein. This β-pleated configuration provides relative resistance to physiological solvents and to conventional proteolysis. There are six types: primary, secondary, hemodialysis-related, hereditary, elderly, and local.
Primary amyloidosis (amyloid light chain, AL) is the most common form of amyloidosis. Automated proteomic analysis of amino acid sequences revealed that these peptides represent the N-terminus of the variable region of the κ or λ light chain of immunoglobulins. Cyclic light chain proteins known as BenceJones proteins, are secreted by a plasma cell clone. AL is associated with a number of plasma cell dysfunctions, such as multiple myeloma and Waldenstrom's macroglobulinemia.
Secondary amyloidosis (AA) is caused by the deposition of AA protein, as a result of proteolytic cleavage of the circulating acute phase reactant, serumamyloid A. AA amyloidosis is associated with disorders infectious, inflammatory or, less commonly, cancer. Rheumatoid arthritis was found in 48% of such patients. In contrast, rates of amyloidosis in rheumatoid arthritis patients ranged from 7% to 21%. Other inflammatory disorders such as Crohn's disease, ankylosing spondylitis, Reiter's syndrome, psoriasis, advanced systemic sclerosis, primary biliary cirrhosis, and serous lupus erythematosus are listed in the underlying diseases. of AA amyloidosis. Other associations include infectious processes such as leprosy, tuberculosis, osteomyelitis, and bronchiectasis; tumors such as renal cell carcinoma, stromal tumor, and intestinal carcinoma; and other disorders, such as idiopathic retroperitoneal fibrosis. Mediterranean fever (FMF) is a rare cause of AA amyloidosis, characterized by recurrent episodes of fever, pleurisy, and peritonitis. In dialysis-associated amyloidosis, the fibroblasts are composed of β2microglobulins, which can be retained in the body by reduced renal clearance.
Geriatric amyloidosis : occurs mainly in patients over 80 years of age and involves the heart, but can also be seen throughout the gastrointestinal tract. Gastrointestinal amyloid is observed in the small and large intestine child veins. Plaques in the brains of patients with Alzheimer's disease are important in the pathogenesis of this disorder.
Hereditary amyloidosis: an autosomal dominant inheritance of amyloidogenic proteins, very rare. The most common form is the variant transthyretin; This deposition leads to increased amyloidotic familial polyneuropathy. On the other hand, there are non-pathological systemic amyloidoses that involve mutations in genes for the apolipoprotein AI, lysozyme, and α-fibrinogen chain. Localized amyloidosis is found in the esophagus, stomach, small intestine, and colon.

Bệnh Crohn là một trong các bệnh cơ bản của bệnh amyloidosis AA
2. Diagnosis of gastrointestinal amyloidosis
Diagnosis is often made long after the onset of symptoms because the presentation is nonspecific and varied, which can mimic many other pathologies. It requires confirmation of the presence of amyloid deposits histologically and is achieved by specific properties after staining with Congo red. The direct rapid magenta staining method can also produce a characteristic red color in normal light, and apple-green birefringence in polarized light indicates prominent mucosal amyloid deposition.
The prevalence of radiological abnormalities is greatest in the small intestine. There may be numerous fine-grained densities or appearance of coarse mucosa, perforation, multiple ulcers, sometimes polyps, erosions, thickening of folds, and impaired motor activity.
Role of endoscopic biopsy
Gastrointestinal screening endoscopic biopsy is diagnosed in most cases of systemic amyloidosis. A variety of mucosal abnormalities are observed in the gastrointestinal tract by endoscopy; Small bowel involvement is particularly common. Lesions may present as mucosal fine granules, granules and nodules, polypoid protrusions, erosions, ulcers, mucosal fibrosis, and intestinal wall thickening. Tada and associates. endoscopically reported gastrointestinal amyloidosis at different sites. In their study, endoscopic findings of the esophagus, stomach, duodenum, and rectum were evaluated in 37 patients with gastrointestinal-related amyloidosis. Endoscopic examination revealed fine granular appearance, convexity, erosion, ulceration, and fibrosis of the mucosa in many cases. These findings are most marked and most frequently noticed in the second part of the duodenum. The frequency of amyloid deposition in the patient samples is as follows; 100% in the duodenum, 95% in the stomach, 91% in the colon and 72% in the esophagus. The degree of amyloid deposition in the duodenum, which is the highest level of the entire gastrointestinal tract, correlates significantly with the frequency of endoscopic findings such as fine grain shapes and protrusions. Therefore, the two endoscopic findings described above are characteristic of this disease and may reflect amyloid deposition in the mucosa or submucosa of the gastrointestinal tract. The results indicate that for the diagnosis of amyloidosis, it is important to examine the upper gastrointestinal tract, especially the duodenum, using endoscopic and biopsy techniques. Macroscopically, AL amyloidosis typically forms protrusions, whereas secondary amyloidosis is characterized primarily by a granular mucosa, as seen in the intestines of the present case.
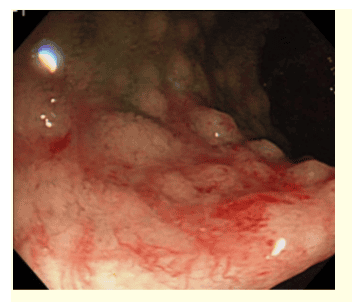
Các tổn thương ở ruột non xuất hiện dưới dạng niêm mạc dạng hạt và nốt, niêm mạc bị bong tróc và xuất huyết ăn mòn.
To visualize the total amount of amyloid in the body, the serum amyloid P component labeled 123 is injected into the circulation. It binds to amyloid fibers in the body. The diagnostic sensitivity of this scan is 90% for AA and AL amyloidosis.
Liver on ultrasound or computed tomography is enlarged with uniform density or echogenicity. Computed tomography may show diffuse or focal areas of hypoattenuation and lack of parenchymal enhancement of the spleen. On magnetic resonance imaging, there is also a uniform intensity with T1 increasing and T2 not changing significantly.
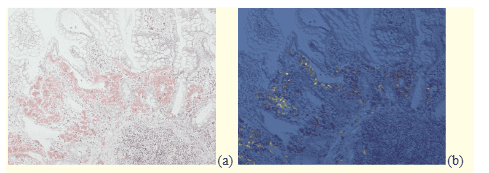
Nhuộm màu đỏ tươi nhanh trực tiếp tạo ra màu đỏ cam đặc trưng trong ánh sáng bình thường (a) và lưỡng chiết màu xanh lá cây táo trong ánh sáng phân cực cho thấy sự lắng đọng amyloid ở niêm mạc nổi bật (b). Nhuộm đỏ nhanh trực tiếp cho thấy nền ít không đặc hiệu hơn so với đỏ Congo.
3. Treatment
Principles of amyloidosis treatment should be directed at the underlying cause and aimed at preventing amyloid accumulation and formation by reducing the abundance of the fibril precursor protein. This approach can help stabilize or improve the function of the affected organ. The goal of primary amyloidosis treatment is to block the synthesis of immunoglobulin light chains by controlling the underlying plasma cell disorder with chemotherapy.
Role of high-dose chemotherapy in combination with hematopoietic stem cell transplantation
Recently, high-dose chemotherapy in combination with hematopoietic stem cell transplantation is being performed for AL amyloidosis with encouraging results. More recently, a patient with severe intestinal amyloidosis secondary to active rheumatoid arthritis was treated with tocilizumab, a humanized anti-interleukin 6 receptor antibody. The treatment resulted in improvement in gastrointestinal symptoms as well as systemic joint pain. Furthermore, her serum AA protein levels returned to normal and repeat endoscopic biopsies revealed no colon amyloid accumulation. Tocilizumab may be a treatment of choice for AA amyloidosis associated with inflammatory arthritis, potentially interfering with the biosynthesis of amyloidogenic precursors induced by the representative proinflammatory cytokine, intereukin 6
New drugs under investigation
Again, a new small molecule inhibitor, R1[6[(R)2carboxypyrrolidin1yl]6oxohexanoyl]pyrrolidine2 carboxylic acid (CPHPC) has been developed to specifically target Serum amyloid P is a common constituent of amyloid deposits and contributes to their formation. CPHPC reduces serum amyloid P levels and prevents amyloid deposition in an open-label proof-of-principle study in systemic amyloidosis.
However, such promising specific agents have so far not been available in the clinical setting of systemic amyloidosis. In fact, the treatment of AA amyloidosis involves controlling the primary disease. For example, long-term anti-tuberculosis therapy has been reported to reduce established amyloidosis. Chlorambucil and tumor necrosis factorα inhibitors against amyloid deposition-induced arthritis. However, the therapeutic effect is anecdotal and inconclusive as shown in sporadic cases or a limited series.
Role of Colchicine
Colchicine, an alkaloid extracted from Colchicum autumnale of the rose family, is prescribed for the treatment of diseases as diverse as gout, Behçet's disease and primary biliary cirrhosis. This drug inhibits microtubule formation, thereby affecting cell mitosis, and may interfere with the phagocytic properties of polymorphonuclear leukemic cells. First, there was an observational case that it was an effective remedy for the prevention of attacks of FMF, an inherited disease characterized by short fevers of serosa, and this was confirmed. by controlled studies. Colchicine is today an effective drug in the prevention and treatment of amyloidosis secondary to FMF. Cases of nephrotic syndrome that resolved after prolonged use of colchicine have been reported not only with FMF but also with ulcerative colitis and ankylosing spondylitis. In a preliminary trial, colchicine (1.5 mg/day) was administered for amyloid nephropathy in patients with hereditary dystrophy epidermolysis bullosa (EB). More recently, we report that gastrointestinal amyloidosis secondary to EB was cured by colchicine at a similar dose 2 months later.
Treatment of gastrointestinal symptoms
Gastrointestinal symptoms are managed with symptom control. It is important to ensure adequate nutrition and enough water. Symptoms of gastroparesis have been effectively treated with metoclopramide or domperidone. Neostigmine may be helpful in alleviating acute colonic obstruction; it can be used as an alternative to colon decompression in patients with various acute pathologies. Diarrhea has been successfully treated with loperamide or octreotide. Total parenteral nutrition is used if the movement disorder-related symptoms are disabling and the patient is malnourished. Antibiotics can be used for bacterial overgrowth. Patients should be supplemented, especially with fat-soluble vitamins. The treatment for gastrointestinal bleeding can be similar to that in other diseases.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.