This is an automatically translated article.
Posted by Specialist Doctor II Phan Phi Tuan - Head of General Surgery Department - General Surgery Department - Vinmec Phu Quoc International General Hospital
Fluids in emergency resuscitation are very important, so the choice of fluid should also be carefully considered. In fact, the choice of fluid in resuscitation has been controversial for a long time, so depending on the patient's case, the appropriate fluid will be indicated.
1. General comments
Management of intravenous fluids has the potential to impact organ function, prognosis, and mortality. Inadequate fluid replacement in the resuscitated patient results in decreased organ perfusion and is associated with decreased oxygen delivery and energy-generating substrates. As a result, the cell must use anaerobic metabolism for energy.
This pathway is both inefficient and produces cytotoxic products. In severe cases, cells can die and the organ is impaired or lost function. Conversely, excessive fluid administration, often with salt, especially in the setting of endothelial dysfunction leading to edema, can also worsen oxygen delivery and impair organ function.
The issue of choosing which fluid (colloid or crystal) is most appropriate for the treatment of hypovolaemia in resuscitation is an important issue and also causes long debate. Supporters of crystallographic resuscitation cite evidence that there is no proven survival benefit, higher cost, and more adverse effects with colloidal resuscitation.
Advocates of colloidal resuscitation demonstrate the need for large volumes of crystalloid to increase plasma volume (at least 3 times colloidal volume), thereby promoting edema and positive fluid balance, both are associated with prognosis and mortality in critically ill patients.
When a choice of alternatives is not agreed on for a long time, often neither option is absolutely correct. Each option is only correct in a particular case.
Isotonic electrolytes that pass freely in the capillary wall should be evenly distributed between the intravascular compartment and the interstitial fluid. Therefore, only about 20-25% of the infused fluid will be retained in the intravascular space. While the particles in the colloidal solution (dd) are larger, they do not penetrate the capillary walls and thus keep the colloidal pressure in the vessel lumen, thus limiting the amount of extravasation. Thus, it may be the best fluid to use to increase intravascular volume. This is theoretically very convincing, but randomized controlled clinical trials in humans have suggested that the volumetric efficiency of colloids is not the theoretical 3-fold of crystalloid but only about 1.3 to 2.1. time.

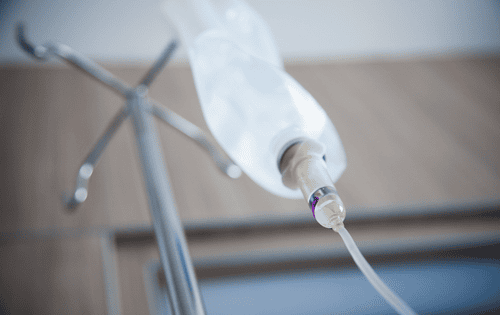
Truyền dịch tĩnh mạch rất quan trọng và cũng gây ra những tranh luận kéo dài
The theory of the advantages of colloidal solutions was questioned as early as the 1970s. However, 30 years later, until large-scale trials were conducted, Saline versus Albumin Fluid Evaluation (Saline versus Albumin Fluid Evaluation). -SAFE ) complete so that final conclusions can be drawn.
The SAFE study compared the efficacy of 4% albumin versus 0.9% NACl in 6 997 critically ill patients and found no difference in all-cause mortality at 28 days. About time spent in resuscitation, hospital stay, mechanical ventilation, and renal replacement therapy. Subgroup analysis also showed that albumin use was associated with an increased risk of mortality in patients with traumatic brain injury. Most recently, a Canadian study of cardiac surgery patients also showed that albumin markedly increased the incidence of acute kidney injury.
To explain this, recent evidence shows that the structure and function of the vascular endothelium in the capillaries really play an important role. In healthy individuals, this membrane is intact, water and electrolytes can pass freely through the endothelium, while protein and large molecules pass through limited by some active transport process.
Therefore, the injected colloid will not escape, so it is kept longer in the vessel. But many different medical conditions can damage the vascular endothelium. The most common cause is an inflammatory response. The systemic inflammatory response alters the endothelial cell phenotype, increasing the size of the pores in the cell, allowing protein to pass through the hole into the interstitial fluid, which is dragged along with water. Therefore, when using colloidal solution, it can also extravasate and cause edema, thereby effectively reducing the volume of colloid compared to the theory.

Truyền dịch keo có khả năng giữ lâu hơn trong lòng mạch hơn
2. Glue solution
There is no discernible benefit to infusion of colloidal solutions compared with crystalline solutions. In contrast, colloidal solutions have generally been shown to increase mortality in traumatic brain injury patients. There is currently no indication for the routine use of colloidal solutions instead of crystals, it is indicated only in rare cases.
Colloidal solutions are sometimes used in wartime conditions, when solutions are not readily available. But this also makes no sense because crystalloids are often easier to obtain than colloids. Colloidal solutions may be used in situations of extreme urgency where blood pressure should be raised even in hemorrhagic shock (primarily intravascular volume depletion) where it is not possible to rapidly infuse large quantities of crystalloids immediately, e.g. get a transmission.
3. Albumin
There is no evidence to support the use of albumin as an emergency resuscitation fluid. Even with the most recent ALBIOS trial, a survival benefit with albumin use was not demonstrated. Because of the high cost and short life of albumin, the use of albumin in resuscitation is not supported.
However, in hypovolemic shock, especially blood loss, prompt restoration of intravascular volume is a priority, a colloidal solution such as 5% albumin (more effective in increasing plasma volume versus crystalloid) is the physiologically best option.
But this idea is also used very little in practice for economic reasons. In cases of volume depletion related to hypoalbuminemia, a small volume of a high colloidal solution such as 25% albumin (which will shift the fluid back to plasma from the interstitial space) is an appropriate option.

Dung dịch albumin có giá thành khá cao
3.1. HES
Research has proven that using HES is not beneficial, on the contrary, it increases harm. Although this colloidal solution did not significantly increase mortality, evidence clearly indicates that HES increases acute kidney injury and increases the use of renal replacement therapy. HES also increases coagulopathy and increases the need for blood transfusions. Therefore, dd HES should not be used in resuscitation.
3.2. Dextran and gelatin
Other synthetic colloidal solutions (dextran and gelatin) are not well studied. Although there is no evidence that these solutions are more harmful than other colloids, there is also no evidence that these solutions are beneficial.
In the absence of strong evidence and because these solutions have the same potential risk as other colloidal solutions, gelatin and dextran should not be used in resuscitation.
Dung dịch Dextran cần được cân nhắc sử dụng kỹ lưỡng trong hồi sức
4. Crystal solution
Although there are also some disadvantages such as the need to infuse large amounts, the possibility of causing interstitial edema, crystalloid solutions are increasingly used because of their ease of availability, low cost, and possible use of large quantities with risks. less than colloid.
4.1. Sugar solution
Sugar solutions are more or less providing energy for the body, but this issue is not of much value in resuscitation. There are different osmotic pressures depending on the concentration.
However, when infused into the body, cells will capture sugar for use, the remaining solution has a very low osmotic pressure, easily crosses both the vascular endothelium and the cell membrane, so it is evenly distributed to the body. fluid compartments in the body. The volumetric effect of 5% sugar is only about 10%, but there is a risk of hyperglycemia, interstitial edema, cell damage due to hypotonicity, and may cause cerebral edema in related diseases, so the sugar solution There is no indication in resuscitation.
It only works as a solvent to mix some incompatible drugs in the case of patients with intravascular excess water, the risk of hypertension. Because in these cases, intravascular fluid should be limited.
Bệnh nhân thừa nước nội mạch cần cần hạn chế dịch nội mạch để tránh tăng huyết áp
4.2. Ringer lactate solution
In cases of hypovolaemia due to dehydration where there is a similar loss of interstitial fluid and plasma as in diarrhea, crystalloids such as Ringer's lactate (uniformly distributed in the extracellular fluid) are appropriate. best.
Sodium chloride 9‰ solution
The use of 9 sodium chloride solution causes metabolic acidosis due to hyperchloremia and increases the risk of acute kidney injury in susceptible patients, especially those with diabetic ketoacidosis. Disconnect the road . This risk can be reduced with the use of equilibrated solutions. Therefore, in this patient population, equilibrated crystalloid solutions should be used instead of 9‰ sodium chloride if possible.
Equilibrium crystal solutions
These solutions did not show any harmful effects in any particular patient population. There is evidence that equilibrium crystals are more beneficial than sodium chloride 9‰ in the prevention of hyperchloremic metabolic acidosis and its consequences.
There are no comparative studies of equilibrated crystalloids. Therefore, there is no consensus regarding the recommendation of a particular equilibria. Current literature supports the use of equilibrated crystals when possible and especially in patients at risk of adverse effects when using 9‰ sodium chloride solution.
Abnormal fluid homeostasis, fluid deficiency or excess fluid are all an important part of many different diseases. The use of fluids has also become central to the treatment of these patients. Although the theory is clear and easy to grasp, in clinical practice it is extremely complex. Therefore, there are many questions raised, many choices are not agreed, many schools are still arguing on forums as well as at the bedside. Infusions must be treated as drugs and therefore require information on their use as well as their pros and cons. Recently, the medical world has emphasized the need to personalize fluid therapy. These questions need to be answered through a close combination of basic science research, applied clinical trials, and large-scale clinical trials.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.