This is an automatically translated article.
Posted by Doctor Mai Vien Phuong - Department of Examination & Internal Medicine, Vinmec Central Park International General Hospital
Esophageal rupture usually occurs after forceful vomiting. This lesion, known as Boerhaave's syndrome, is a tear through the wall of the esophagus. The disease can cause complications of mediastinitis, sepsis, mortality rate about 35%.
1.Introduction to Boerhaave Syndrome
Boerhaave syndrome is one of the most fatal gastrointestinal disorders, with a mortality rate of up to 40%. Symptoms can vary and diagnosis can be difficult. In addition, a number of factors, including difficulty assessing the esophagus and abnormal blood supply of the organ, contribute to the high incidence of this condition. Without treatment, the survival time of Boerhaave syndrome can be several days. Management relies on prompt recognition and intervention, as lack of therapeutic interventions can be fatal.
Boerhaave's syndrome is caused by rupture of the esophagus due to excessive vomiting. The disorder may present with vague symptoms or the classic Mackler triad of vomiting, chest pain, and subcutaneous emphysema (pneumothorax). The earlier the diagnosis, the better the outcome.
Hình ảnh rách thực quản do nôn ói quá nhanh và mạnh
2.Causes of Boerhaave's Syndrome
Boerhaave syndrome is also known as spontaneous esophageal rupture or exercise-induced rupture of the esophagus. Although vomiting is thought to be the most common cause, other causes include weightlifting, defecation, epileptic seizures, abdominal trauma, pneumatic trauma, and childbirth, all of which can increase pressure in the esophagus and cause pressure esophageal rupture. Most cases occur in patients with a normal lower esophagus, although the presence of inflammation or ulceration of the esophagus has also been found in a small number of individuals.
Two common risk factors include alcoholism and bulimia.
3.Epidemiology of Boerhaave's syndrome
Boerhaave syndrome was first described in 1724 by Hermann Boerhaave, Professor of Medicine at Leiden University. In one of his publications entitled “History of a previously uncharacted neurological disease”, he discussed the case of Baron Jan von Wassenaer, a Dutch admiral who later party, began vomiting and left chest pain soon after. Unfortunately, he only survived for 24 hours after the incident. Today, Boerhaave syndrome accounts for about 15% of all cases of esophageal rupture. Although the actual incidence of esophageal perforation worldwide is unclear, some studies estimate the incidence to be around 3.1 per 1,000,000 per year. The patient population with Boerhaave syndrome varies, but the risk is highest in middle-aged men. This condition has a lot to do with drinking.
4.Pathophysiology
Spontaneous esophageal rupture is caused by a sudden increase in intraesophageal pressure, resulting in a complete transesophageal laceration. Complications will depend on the site of the rupture because the esophagus is adjacent to different areas of the body. The middle esophagus is adjacent to the right pleura while the lower esophagus is adjacent to the left pleura. Rupture occurs most commonly in the left posterior wall of the distal third of the esophagus with extension into the left pleural space. Esophageal perforations in the thorax can lead to mediastinitis, emphysema, or gangrene as gastric contents enter this area. However, rupture can also occur in the neck or upper chest area. Perforations in the upper chest or middle of the esophagus tend to produce pleural effusion or pneumothorax on the right side.
Nôn ói nhanh và mạnh là nguyên nhân chính gây ra hội chứng Boerhaave
5.Signs of disease detection
A typical case of esophageal rupture often presents with Mackler's triad, including: repeated vomiting, often seen in middle-aged men with a high diet and alcohol consumption; chest pain: sudden onset after vomiting, pain in the lower chest and upper abdomen, pain may radiate to the left shoulder or back, pain increases when swallowing; subcutaneous emphysema: this is a common symptom in 28-66% of patients and is very helpful in helping to confirm the diagnosis. Computed tomography showed pleural effusion, pneumothorax, mediastinal pneumothorax. However, the symptoms can vary depending on the location of the injury, the time from the rupture of the esophagus to the time of intervention, some symptoms may be: fever, sweating, purple skin, heart rate rapidly, blood pressure drops. Vomiting blood: although rare, if present, this symptom helps to differentiate from Mallory-Weiss syndrome. Cough usually occurs after swallowing, because there is communication between the esophagus and the pleural space. Shortness of breath, rapid breathing, due to pleurisy or pleural effusion. Hoarseness. Stiff abdomen. For patients who come late, often have signs of infection, sepsis, so diagnosis in this period is quite difficult when infectious complications have masked other manifestations on imaging. Therefore, early diagnosis of Boerhaave syndrome is crucial to saving the patient's life. In fact, about 30% of cases of esophageal perforation have atypical clinical presentation. The diagnosis of Boerhaave's syndrome can be challenging because the symptoms are often atypical and present late, leading to a mortality rate of about 35%, making this syndrome the deadliest disease of the ureteral perforation. chemical.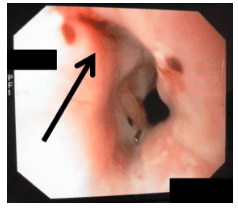
Một trường hợp bị hội chứng Boerhaave được nhìn thấy trên nội soi
Vinmec International General Hospital is a high-quality medical facility in Vietnam with a team of highly qualified medical professionals, well-trained, domestic and foreign, and experienced.
A system of modern and advanced medical equipment, possessing many of the best machines in the world, helping to detect many difficult and dangerous diseases in a short time, supporting the diagnosis and treatment of doctors the most effective. The hospital space is designed according to 5-star hotel standards, giving patients comfort, friendliness and peace of mind.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.