This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital
Artificial Intelligence – AI is the English term for artificial intelligence, a computer technology that is developing and widely used in the medical field to improve work efficiency. Currently, the applications of artificial intelligence AI in the diagnosis of esophageal cancer are being studied and recorded.
1.What is Artificial Intelligence? Artificial Intelligence (AI: Artificial Intelligence) can be defined as a branch of computer science that deals with the automation of intelligent behaviors. AI is a part of computer science, so it must be based on solid, applicable theories and principles of this field.
2. What is the difference between artificial intelligence AI, Machine Learning and Deep Learning? Artificial intelligence is the study of how to build machines capable of performing tasks that normally require human intelligence. AI (Artificial Intelligence) covers many areas of research, from genetic algorithms to expert systems, and provides scope for arguments about what constitutes AI.
Machine Learning is the process of teaching a computer to perform a task, instead of programming it how to perform that task step by step. Deep Learning is a subset of Machine Learning, capable of being different in some important respects from traditional shallow Machine Learning, allowing computers to solve a wide range of unsolvable complex problems.

Hình 1: Trí tuệ nhân tạo AI ngày càng được ứng dụng nhiều trong y học
3. Overview of the application of artificial intelligence to gastrointestinal endoscopy Due to the rapid progression and poor prognosis of esophageal cancer (EC), early detection and diagnosis of esophageal cancer is valuable. greatly in improving the patient's prognosis. However, early endoscopic detection of esophageal cancer, especially Barrett dysplasia or esophageal squamous dysplasia, is difficult. Therefore, the requirement for more effective methods of detecting early esophageal cancer features has led to intensive research in the field of artificial intelligence (AI). Deep learning (DL) has brought about breakthroughs in image, video and other aspects of processing, while complex neural networks (CNNs) have paved the way for detect high-resolution endoscopic images and videos.
4. Introduction to Esophageal Cancer Esophageal cancer (EC) is the eighth most common cancer and the sixth leading cause of cancer death worldwide. Esophageal cancers mainly include esophageal adenocarcinoma (EAC) and esophageal squamous cell carcinoma (ESCC). Esophageal adenocarcinoma is the most common disease in Western countries, more than 40% of patients with esophageal adenocarcinoma are diagnosed after the disease has metastasized, and the 5-year survival rate is less than 5 years. 20%.
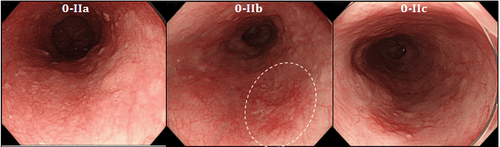
Hình 2: Ung thư thực quản giai đoạn sớm được nhìn thấy qua nội soi
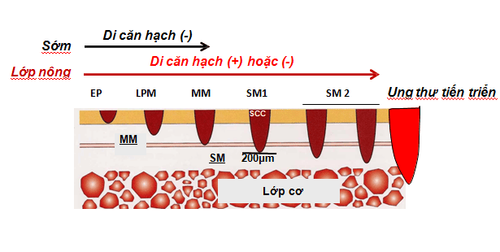
Hình 3: Phân chia giai đoạn của ung thư sớm thực quản
4.1 Barrett's esophagus (BE) Barrett's esophagus (BE) is a premalignant condition characterized by the replacement of the normal squamous esophageal epithelium with metaplastic intestinal epithelium containing goblet cells. This is the result of chronic inflammation of the esophagus, which increases the risk of esophageal adenocarcinoma. Endoscopic follow-up of patients with Barrett's esophagus for early detection of dysplasia or carcinoma has been recommended by the Western Gastrointestinal Association. Endoscopic follow-up in patients with Barrett's esophagus is required with random 4-quadrant biopsies obtained every 1 to 2 cm to detect dysplasia. This method is invasive, time consuming, and difficult to adhere to.
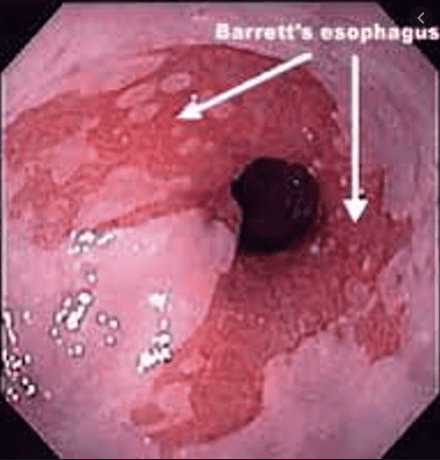
Hình 4: Hình ảnh Barrett's thực quản
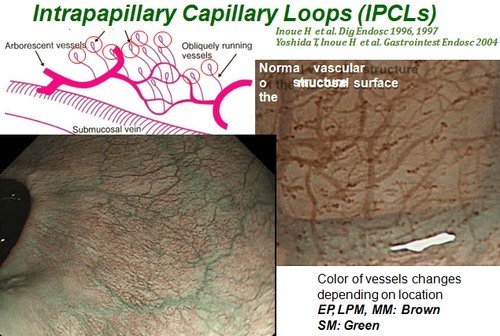
5. Role of esophagogastroduodenoscopy in the diagnosis of early esophageal cancer Gastroscopy remains the primary way to detect early ESCC. However, the endoscopic features of these early lesions are subtle and easily missed compared with conventional white light endoscopy (WLE). Endocardial capillary loops (IPCLs), which are microvessels, are considered to be hallmarks of ESCC esophageal squamous cell carcinoma, because their morphological changes correlate with depth of invasion. esophageal squamous cell carcinoma. Advanced endoscopic imaging modalities, such as endoscopic narrow-band imaging (NBI), combined with magnified endoscopy, help improve imaging of cellular microvascular patterns in the lining of the esophagus of patients with esophageal squamous cell carcinoma. Although NBI has shown high sensitivity in detecting esophageal squamous cell carcinoma, its effectiveness in identifying these lesions is still limited.
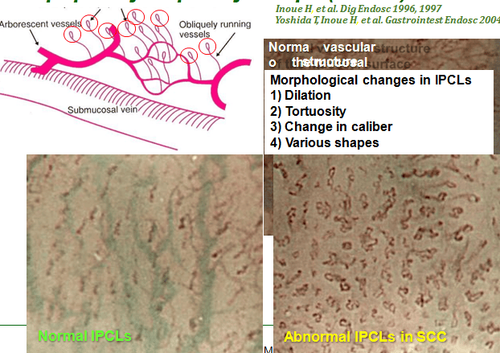
Hình 5: Hình ảnh các quai mao mạch trong ung thư thực quản
6. Application of Machine learning and Deep learning algorithms in esophageal cancer The demand for more effective methods of early detection and characterization of esophageal cancer has led to in-depth studies in the field artificial intelligence (AI), which can be identified by machine-established intelligence as opposed to the natural intelligence displayed by humans and other animals. Machine learning (ML) and deep learning (DL) are important parts of AI. Machine learning can be divided into supervised and unsupervised methods. Unsupervised learning is to identify groups in data according to commonalities, lacking knowledge of the number of groups or their meanings. When the training package contains pairs of inputs, the output needs a supervised learning model to map the new input to the output. Conventional ML techniques are limited in their ability to process natural data in its raw form. In the early stages of research and development, model training was mainly with ML, through which researchers had to manually extract probable disease features based on clinical knowledge. The power of this computer-aided diagnosis (CAD) system is weak and insufficient to apply in clinical real-time diagnosis.
7. Role of a Convolutional Neural Network (CNN) A Convolutional Neural Network (CNN) is a supervised machine learning model inspired by the visual cortex of the human brain that processes and recognizes images . Each artificial neuron is a computational unit and all of them are interconnected, forming a network. Using multiple network layers, CNN can extract key features from an image with minimal pre-processing and then provide final classification through fully connected layers as output. The increasing competition for performance has led to the increasing complexity of pooling layers which led to the concept of deep learning. The important aspect of deep learning is that these feature classes are not designed by human engineers. They are learned from data using a general-purpose learning process. Deep learning has brought breakthroughs in image, video and other aspects of processing, while iterative CNNs have shed light on the detection of endoscopic images and videos.
8. The role of AI artificial intelligence in early esophageal cancer detection AI AI is based on white light endoscopy (WLE) system and NBI narrowband endoscopy system. There are some limitations to recognizing early cancerous lesions associated with Barrett's esophagus by WLE, a common technology. High-definition WLE (HD-WLE) and the NBI endoscopy system were once considered to improve the accuracy of diagnosing early cancerous lesions associated with Barrett's esophagus. However, the improvement has not yet satisfied the endoscopists. This situation stimulated the development of a CAD system for early cancerous lesions in Barrett's esophagus based on a supervised ML blood learning algorithm.
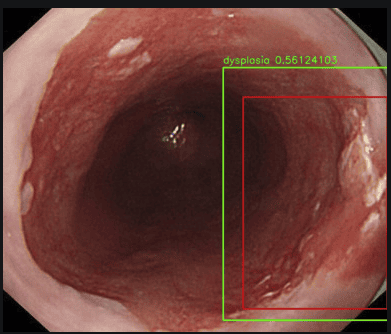
Hình 6: Hình ảnh loạn sản thực quản được đánh giá qua hệ thống nội soi có sử dụng trí tuệ nhân tạo AI, máy tính sẽ tìm khu trú tổn thương tự động (ô màu đỏ), đánh giá tổn thương đó có bao nhiêu phần trăm là ung thư
AI artificial intelligence based on endoscopic optical tomography and confocal laser endoscopy. In addition to WLE and NBI, endoscopic coherence optical tomography (EOCT) and endoscopic confocal laser (CLE) are also used for early diagnosis of EAC/BE-associated dysplasia. EOCT can identify early tumor lesions associated with Barrett's esophagus by analyzing mucosal and submucosal structures of the esophagus. CLE can observe mucosal tissue and cell morphology to achieve optical biopsies. However, the complexity of these two imaging technologies, the time-consuming reading of images, and the requirement for highly skilled internists limit their clinical use. To solve this problem, Qi et al extracted multiple EOCT imaging features and combined one or more features to classify lesions, but the results were not satisfactory. Then, Swagger et al used volumetric laser endoscopic imaging (VLE, integrated with second-generation OCT) for training and testing, and the results showed that the CAD system was superior to other models. VLE experts.
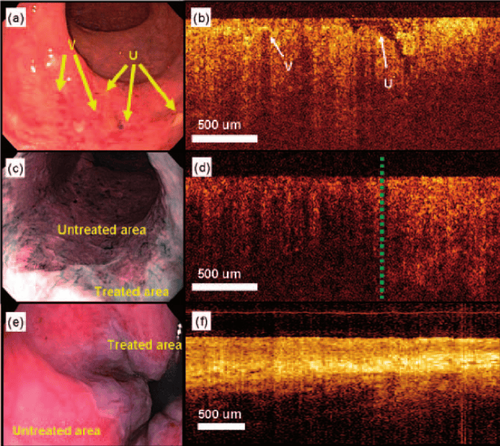
Hình 7: Hình ảnh của chụp cắt lớp quang kết hợp qua nội soi (EOCT) và nội soi bằng laser đồng tiêu (CLE)
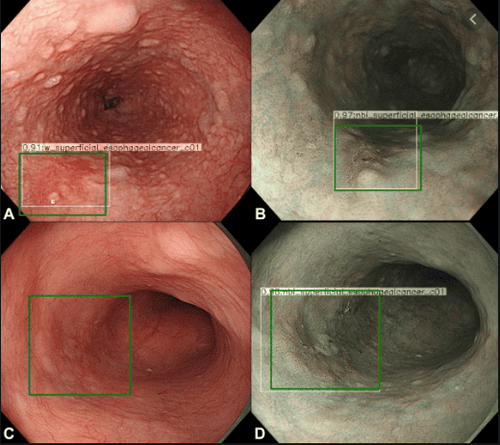
Hình 8: Sử dụng AI trong hệ thống nội soi: Ô vuông màu xanh là máy tính tự động khu trú hình ảnh tổn thương khi đưa máy soi đến.
Hình 9: Hình ảnh rằng cấu trúc quai mao mạch IPCL được nhìn thấy trên nội soi NBI
10. The role of AI in endoscopy AI AI is based on high-resolution microscopy and endoscopy. Endoscopic endoscopy (endoscopy at the cellular level) is a new technology that combines magnified endoscopy with vital staining. Due to the excellent magnification, the endoscope can clearly visualize the epithelial cells of the esophageal mucosa to achieve an effect similar to the diagnosis of pathology. However, if endoscopists want to use endoscopy to independently complete real-time detection, they need a strong background in pathology, which is clearly impractical. Therefore, AI may be the best choice to aid in endoscopic diagnosis. Kumagai et al. have shown that the performance of the system using higher magnification images is better than the system using lower magnification images. However, no stratified analysis of superficial and advanced esophageal cancer was included in this study. The results may not accurately reflect the ability of endoscopy combined with AI to diagnose early esophageal cancer. High-resolution microscopy (HRME) can be used to observe esophageal mucosal tissue and cell morphology. Shin et al tested the ability of different imaging features to distinguish tumors from non-tumor lesions, and the best features were selected with 84% sensitivity and 95% specificity. .
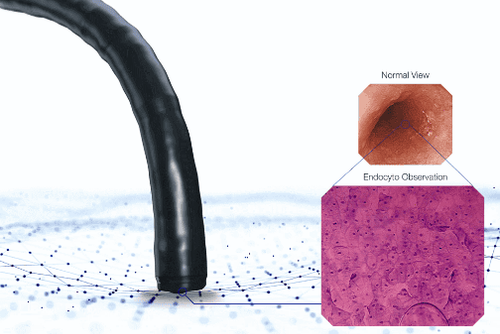
Hình 10: Hình ảnh nội soi tế bào
11. Role of AI in histopathological diagnosis of early esophageal cancer Although AI combined with endoscopic diagnosis has made great progress, endoscopic diagnosis still cannot replace the gold standard in disease diagnosis. physical. However, there is a problem in the pathological diagnosis of early esophageal neoplasia i.e., the accuracy of the diagnosis of dysplasia is not ideal with significant variation between the host of observations. To address this issue, Sabo et al established two models to distinguish non-dysplasia (ND) from low-grade dysplasia (LGD) and LGD from high-grade dysplasia (HGD) by image extraction. pathological sections stained with hematoxylin and eosin (HE). The results showed that the two models performed well in the diagnosis of indistinguishable contour lesions. Baak et al combined the HE-stained pathologic cross-sectional imaging features with immunohistochemical indices P53/Ki67 and used endoscopic gastrointestinal resection specimens and biopsies. Barrett's esophagus for testing. It was found that the system performed well in distinguishing ND from LGD and LGD from HGD, however the accuracy of distinguishing HGD from intramucosal carcinoma needs to be improved. The performance of the system is better than that of the general pathologist and only slightly worse than that of the experienced pathologist.
12. Role of AI in genetic diagnosis of early esophageal cancer As mentioned above, the invasiveness of endoscopic diagnosis and the variability of pathological diagnosis, together with recent advances in The pathogenesis of esophageal cancer, and the development of different omics technologies, have made early EC gene diagnosis a hot research topic. Zhang et al and Yu et al used microRNAs and long noncoding RNAs specifically expressed in patients with esophageal squamous cell carcinoma to establish diagnostic models, and the results showed that both Both can be used to effectively differentiate early from advanced tumours.
12.1 Role of AI in Risk Stratification of Early Esophageal Cancer It is estimated that only 0.12% -0.43% of Barrett's esophagus patients may progress to early esophageal cancer each year, It is particularly important to establish an efficient model to predict the annual risk of early esophageal cancer in patients with Barrett's esophagus. Previously risk stratification was based primarily on the presence of dysplasia, but its efficacy was not ideal. Critchley-Thorne et al established a predictive model based on characteristic differences in immunofluorescence markers and histopathology between Barrett's esophagus patients who developed early esophageal cancer. per year and those who do not have the disease. Results have not been encouraging, with more than 30% of Barrett's esophagus patients developing early esophageal cancer each year classified as low-risk. Li et al established a prediction model based on single nucleotide polymorphism differences in the biopsy tissues of Barrett's esophagus patients with good performance to predict early esophageal cancer each year.
In conclusion, AI artificial intelligence is trying to be used for endoscopic detection, pathological diagnosis, genetic diagnosis and cancer risk prediction of early esophageal cancer. It is useful for endoscopists and pathologists to improve diagnostic accuracy and assist physicians in treatment and follow-up strategies.
Undeniably, AI artificial intelligence is very useful for endoscopists and pathologists to improve diagnostic accuracy to aid in treatment and provide follow-up strategies with the goal of The ultimate goal is to improve the patient's quality of life.
Actively screening for gastrointestinal cancer is the best and scientific method for early detection of gastrointestinal cancers, including common cancers such as esophageal cancer, stomach cancer, and gastric cancer. colon cancer. Vinmec International General Hospital currently has a package of screening and early detection of gastrointestinal cancer that combines clinical and paraclinical examination to bring about the most accurate results possible.
In addition to being performed by a team of experts and experienced doctors, patients will receive a gastroscopy, colonoscopy with an NBI endoscope with anesthesia. Peripheral blood cell total analysis (by laser counter). Automated prothrombin time test. Activated Partial Thromboplastin Time (APTT) test using an automated machine. General abdominal ultrasound... The application of technology and modern equipment to the examination will give accurate results, make the treatment more effective, and shorten the hospital stay for the patient. core.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424. [PubMed] [DOI]2. Hur C, Miller M, Kong CY, Dowling EC, Nattinger KJ, Dunn M, Feuer EJ. Trends in esophageal adenocarcinoma incidence and mortality. Cancer. 2013;119:1149-1158. [PubMed] [DOI]
3. Thrift AP. The epidemic of oesophageal carcinoma: Where are we now? Cancer Epidemiol. 2016;41:88-95. [PubMed] [DOI]
4. Lu-Ming Huang, Wen-Juan Yang, Zhi-Yin Huang, Cheng-Wei Tang, Jing Li, Artificial intelligence technique in detection of early esophageal cancer, World J Gastroenterol. Oct 21, 2020; 26(39): 5959-5969