This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II Nguyen Binh - Department of General Surgery - Vinmec Ha Long International Hospital.Colon bulge is caused by a lack of ganglion cells at the end of the colon, making it difficult for patients to defecate. And laparoscopic surgery is the most common treatment method today. The following article will provide readers with the necessary information related to anesthesia for laparoscopic surgery for congenital colonic aneurysms.
1. Diagnosis of congenital megacolon
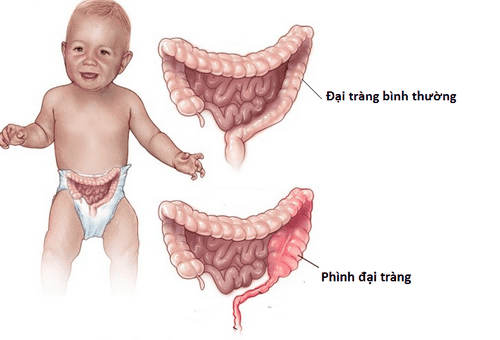
Congenital megacolon, also known as congenital colonic agranulomatosis or Hirschsprung, occurs in young children including both boys and girls. This congenital disease is in about 15% of common diseases and birth defects, requiring surgery for timely treatment.The prominent manifestation of congenital megacolon in young children is the fact that the patient has extremely difficult bowel movements, if not treated quickly, this condition will get worse, even if The patient has soft stools.
This disease causes children to become increasingly anorexic, slow to grow. Not only that, there are many cases of patients experiencing extremely dangerous complications such as intestinal obstruction, severe enteritis, making the care of children with an enlarged colon even more difficult.
Currently, with the development of medicine, this disease can be completely cured by laparoscopic surgery for congenital megacolon. But before giving the most accurate diagnosis, the patient will be asked to perform a number of mandatory tests such as:
X-ray: X-ray technique using additional contrast material is often required. required for the diagnosis of congenital megacolon in infants. Based on this technique, the specialist can easily see the narrow bowel segments as well as the dilated bowel segments of the patient. This technique tests the control of the muscles around the rectum, but is not commonly used. Using a colon sample to do necessary tests (aspiration biopsy, sample biopsy): these are considered to be the tests that bring the highest accuracy to diagnose the disease. Thanks to that, the doctor can make a final conclusion whether the baby is suffering from congenital megacolon.

Phình đại tràng bẩm sinh khiến trẻ ngày càng trở nên biếng ăn, chậm lớn
2. Anesthesia for laparoscopic surgery for congenital megacolon
2.1 Preparation Performers: doctors and nurses of the emergency resuscitation department.Facilities:
System of anesthesia machines with breathing, providing hand-held oxygen, along with accurate monitoring of vital functions (including ECG, SpO2, EtCO2, arterial blood pressure, breathing rate) , temperature), suction machine, defibrillator... Laryngoscope, suction tube, mask, endotracheal tube of all sizes, squeeze ball, Magill pliers, soft mandrin, oropharyngeal cannula. Lidocaine 10% spray, and salbutamol spray. Prophylactic means for difficult intubation: laryngeal mask, Cook tube, tracheostomy kit, flexible bronchoscope, mouth opening pliers... 2.2 Procedures Check patient records; Check the patient's health status; Technical implementation. General steps:
Standard position of the patient: lying on his back, breathing 100% oxygen at 3-6 l/min before induction of anesthesia at least 5 minutes; Install patient monitoring machine; Establish an efficient transmission line; Apply pre-anesthesia (if necessary). Induction of anesthesia:
Commonly used sleeping pills are: intravenous anesthetics (etomidat, thiopental, ketamine...), or volatile anesthetics (sevoflurane...); Pain relievers such as: fentanyl, sufentanil, morphine...; Muscle relaxants (if necessary): succinylcholine, rocuronium, vecuronium..; Conditions for endotracheal intubation are allowed when: the patient is in deep sleep, has enough standard muscle relaxation (almost all cases); Two common techniques for intubation are: nasal or oral. Here is the technique of tracheal intubation through the mouth, readers can refer to it more:
Open the patient's mouth, the laryngoscope is slowly inserted into the right side of the mouth, pushing the patient's tongue to the left side, push the lamp deep, the right hand simultaneously presses the cricoid cartilage to search for the glottis and epiglottis; Rapid induction of anesthesia and the Sellick maneuver for full stomachs; Insert the endotracheal tube gently through the area of the glottis, and stop only when the balloon of the endotracheal tube has passed through the vocal cords by 2-3 cm; The laryngoscope can be withdrawn gently; Then inflate the endotracheal balloon; Check the current position of the endotracheal tube in the body by listening to the lungs and using EtCO2 results; Fix the tube with adhesive tape; Place the cannula in the patient's mouth to avoid biting the tube (if necessary).
3. Complications and treatment

Sau phẫu thuật bệnh nhi có thể gặp một số tai biến về hô hấp
3.2 Hemodynamic Disorders Hemodynamic disorders are cases in which the patient has arrhythmia, hypo or hyperglycemia. Treatment can be based on specific symptoms and causes.
3.3 Respiratory complications The patient is bent, retracted or the endotracheal tube is pushed deep into the lungs, leading to an opening of the respiratory system, causing oxygen depletion. These situations can be resolved by quickly ventilating and re-supplying 100% oxygen, and then finding and addressing the cause.
Thus, through this article, readers have learned important information related to the anesthetic process for laparoscopic surgery for congenital colonic aneurysms. To be diagnosed and find the best treatment, pediatric patients should be taken to reputable medical centers for timely examination.
As a key area of Vinmec Medical system, Pediatrics Department always brings satisfaction to customers and is highly appreciated by industry experts with:
Gathering a team of leading pediatricians: including leading experts with high professional qualifications (professors, associate professors, doctorates, masters), experienced, worked at major hospitals such as Bach Mai, 108.. Doctors All are well-trained, professional, with a mind - range, understanding young psychology. In addition to domestic pediatric specialists, the Department of Pediatrics also has the participation of foreign experts (Japan, Singapore, Australia, USA) who are always pioneers in applying the latest and most effective treatment regimens. . Comprehensive services: In the field of Pediatrics, Vinmec provides a series of continuous medical examination and treatment services from Newborn to Pediatric and Vaccine,... according to international standards to help parents take care of their baby's health from birth to childhood. from birth to adulthood Specialized techniques: Vinmec has successfully deployed many specialized techniques to make the treatment of difficult diseases in Pediatrics more effective: neurosurgery - skull surgery, stem cell transplantation. blood in cancer treatment. Professional care: In addition to understanding children's psychology, Vinmec also pays special attention to the children's play space, helping them to have fun and get used to the hospital's environment, cooperate in treatment, improve the efficiency of medical treatment. Dr. Nguyen Binh has more than 20 years of experience in the field of anesthesia - resuscitation in thoracic surgery, anesthesia resuscitation for elderly patients... Currently a Doctor of General Surgery, International General Hospital Vinmec Ha Long.
To register for examination and treatment with pediatricians at Vinmec International General Hospital, please click the "Contact Us" button on the website or register online HERE.
MORE:
Diagnosis and treatment of congenital megacolon in children Congenital megacolon in children: Causes and signs to recognize Megacolon laparoscopic surgery (one-stage anal Soave surgery)