This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Nguyen Trung Hau - Doctor of Odonto-Stomatology - Department of Medical Examination & Internal Medicine - Vinmec Da Nang International General Hospital. BSCK I Nguyen Trung Hau has more than 10 years of experience working in the field of Odonto-Stomatology, Dr. Hau is especially experienced in maxillofacial surgery, cosmetic dentistry, and Implant implants.Trauma treatment has evolved significantly over the past few decades thereby reducing the golden hour mortality rate. However, challenges remain, and one such area is maxillofacial trauma in patients. Severe trauma to the maxillofacial region can complicate the early management of trauma patients because of the proximity of the brain, cervical spine, and airway.
1. Maxillofacial trauma
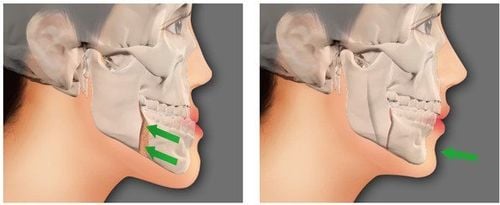
Gãy xương có thể gây tổn thương hàm mặt
Safe and optimal airway management for patients with maxillofacial trauma requires an appreciation of the nature of the injury. There are some maxillofacial injuries that require immediate treatment, especially in acute upper respiratory tract injury or when bleeding is diffuse. According to Hutchison et al, there are six specific situations associated with maxillofacial trauma that may adversely affect the airway:
Posterior displacement of the fractured maxillar parallel to the inclined plane of the skull base may block the pathway. nasopharyngeal breathing. A bilateral fracture of the anterior mandibular can cause a symphysis fracture and the tongue to slide posteriorly and block the pharynx in the supine patient. Broken or chipped teeth, bone fragments, vomit, blood and secretions, and foreign bodies, such as dentures, debris, and shrapnel, can block the airway anywhere along the nasopharynx and larynx . Bleeding from blood vessels inside the wound or severe nosebleeds can also contribute to airway obstruction. Soft tissue swelling and edema caused by head and neck trauma can damage the airways. Trauma to the larynx and trachea can cause swelling and displacement of structures, such as the epithelium, arytenoid cartilage, and vocal cords, thereby increasing the risk of airway obstruction.
2. Control the airway
Kiểm soát đường thở sớm là tiền oxy hóa, có thể kéo dài khoảng thời gian lên đến trạng thái thiếu oxy
Therefore, life-saving intervention should begin with airway resuscitation, when needed. In fact, the most common critical care errors that contribute to injury patient mortality are related to airway and respiratory management. Issues with airway control are not limited to the early stages of the procedure anywhere to resuscitate the patient.
The first action in early airway control is pre-oxygenation, which can prolong the period up to hypoxia. Effective pre-oxygenation of the lungs increases the oxygen content in functional residual capacity, which is the primary oxygen storage site during apnea.
Because time to achieve airway control before dangerous levels of hypoxia begin to be critical, preoxygenation is critical and must be performed as much as possible, using a non-respiratory respirator. treatment. In some patients, preoxygenation is not feasible due to maxillofacial trauma, and hypoxia would be expected.
Intubation is the gold standard procedure to secure the airway in trauma patients. It is administered orally with rapid sequential induction and manual straight-line stabilizing manipulation, to reduce the risk of pulmonary aspiration and to account for cervical spine injury. However, intubation is expected to be difficult in a maxillofacial trauma patient.
Regarding mask ventilation, mask ventilation is problematic in patients with maxillofacial trauma because the oral cavity or pharyngeal anatomy can be disturbed by trauma and blocked by bleeding. Therefore, the respirator cannot be fitted to the face for effective mask ventilation. Furthermore, an injured airway can prevent air from effectively moving from the mask into the lungs.
3. Airway control device
There are many devices that control the airways; however, only an endotracheal tube or tracheostomy tube is considered definitive when applicable. Several airway devices are beneficial in the management of patients with maxillofacial trauma:Flexible fiber optic bronchoscope (FOB): Although fiber optic intubation is performed under local anesthesia to Achieving successful intubation is one of the recommended methods in situations where airway control is difficult. Video laryngoscopes: such as the GlideScope video laryngoscope, allow indirect viewing of the epiglottis and vocal cords. The successful use of video laryngoscopes, based on a good view of the internal airways, is prevented in patients with blood and exudate trauma. Supraglottic airway devices (SADs), such as the LMA and several of its diverse variants, are critical devices for difficult airway management. For airway management of trauma patients, SAD is placed in the nasopharynx and its successful placement requires a high level of experience. In addition, patients with facial trauma often have minimal space in the mouth, which complicates the use of a supraglottic airway device.
4. Airway surgery
Airway surgery is used to control the airway as a last resort; however, in patients with maxillofacial trauma it is sometimes the best solution.Surgical technique:
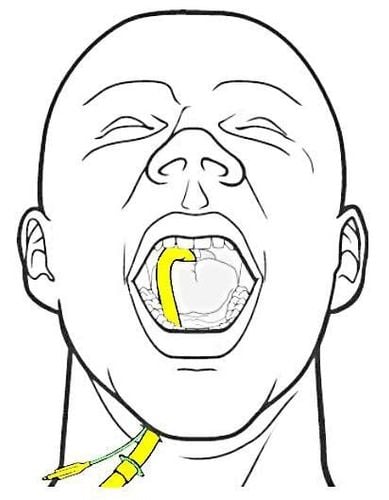
Percutaneous endotracheal intubation under the chin requires the use of an enhanced spring endotracheal tube to avoid folding of the tube during use. After intubation, a 2cm incision was made between the chin and the mandibular angle and dissection to the floor of the mouth. The incision is made through the superficial fascia, the platysma, and the deep fascia. An opening in the floor of the mouth. At the end of dissection, it is necessary to open the clamp/forcep to tunnel the tube through without further intervention. When the incision is complete, pull the tube through the tunnel in a gentle rotating motion. Then, connect the tube to the ventilator and sew the tube in place. When indicated, extubation of the endotracheal tube will be performed through an external incision: release the intermaxillary fixation, remove the fixation wire, and disconnect the tube from the ventilator. Pull the tube back into the oral cavity and reconnect it to the anesthetic machine. At this point, the patient is ventilated via an oral endotracheal tube and extubation will be performed as usual.
Performing a tracheostomy or tracheostomy under local anesthesia is a life-saving procedure in selected hospital-acquired patients who cannot be intubated, unable to breathe. Airway surgery is a safe method to protect the airway when the procedure is performed by an experienced surgeon. However, this method has disadvantages:
It has a 6% complication rate such as hemorrhage or pneumothorax. This procedure can be difficult to do in an emergency or urgent situation, and the procedure can sometimes be fatal. When tracheostomy is performed under local anesthesia, it causes discomfort or even pain to patients who may already be experiencing severe pain and anxiety. Patients with difficult airways are also at increased risk of postoperative complications. After surgery, mucous membranes become edematous, soft tissues swell, and the airways may become compressed.
Highly skilled medical staff and many advanced airway control devices are required to manage patients with maxillofacial trauma. Good coordination between surgeons, anesthesiologists and trauma specialists with the contribution of expert knowledge is key to better patient improvement.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.