This is an automatically translated article.
Acute bronchial asthma is a chronic respiratory disease, common in adults and children. Acute asthma attacks usually occur at night, most of which are short-lived. If severe asthma attacks are left untreated, they can lead to death.
1. Acute bronchial asthma
Asthma is a chronic inflammatory disease of the airways caused by many cells and cellular components. Asthma increases airway responsiveness including: constriction, increased sputum secretion, obstructive edema, airway restriction. As a result, the patient will have symptoms of wheezing, shortness of breath, chest tightness and repeated coughing. Cough usually occurs early in the morning and at night, and can be resolved spontaneously or with medication.
Asthma, if not diagnosed and treated, can lead to complications including:
Pneumothorax Infection of the lungs, bronchial atelectasis Pulmonary atresia thoracic complications of treatment such as pseudo-cushing syndrome due to corticosteroid therapy

Suy hô hấp là biến chứng của hen phế quản
2. Diagnosis of bronchial asthma
2.1 Definitive diagnosis To definitively diagnose acute bronchial asthma in adults, the doctor will rely on the medical history, symptoms and laboratory test results.
History, medical history
Patient and family history of allergic diseases eg: urticaria, eczema, allergic rhinitis or diagnosed asthma
Atopy Organ: bronchial asthma is common in people with predisposing factors. The site is sensitive to allergens and environmental agents. History of respiratory disease: recurrent pneumonia, bronchiolitis at a young age. History of ENT diseases: allergic rhinitis, nasal polyps, purulent sinusitis. Digestive diseases: food allergies, gastro-intestinal reflux. Skin diseases: eczema, urticaria, atopic dermatitis. Family: has Atopy and has bronchial asthma.

Bệnh lý ngoài da có liên quan đến hen phế quản
Symptoms
Abnormal murmurs: Abnormal murmurs are heard in the lungs, during dyspnea with crackles, snoring Cough: often uncharacteristic, dry cough; sometimes white, viscous, sticky sputum (pearls); cough usually after shortness of breath subsides. Some patients have a cough as the sole symptom of an outbreak: a persistent, recurrent, nocturnal cough that constitutes the only cough form of bronchial asthma. Shortness of breath: this is the basic and characteristic symptom of an outbreak. Often severe dyspnea, dyspnea, accompanied by hissing sound, often at night and in the morning. Intermittent, recurrent dyspnoea with weekly, monthly or seasonal cycles or when exposed to allergens, infections, or exercise. Shortness of breath, severe or mild in episodes, may resolve on its own or with bronchodilators. There are cases of persistent dyspnea, continuous or no dyspnea, creating an atypical clinical form. Chest congestion: the patient feels stuffy or squeezing in the chest. Symptoms increase with dyspnea and decrease with cessation of dyspnea. Laboratory tests
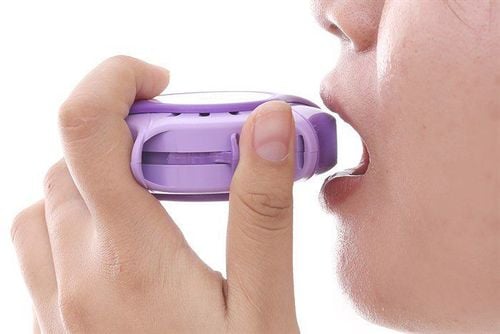
Measure peak expiratory flow by flowmeter in the diagnosis of asthma, if the result is equal to or greater than 20% of the pre-medication level or the peak expiratory flow rate changes by or equal to or More than 20% In addition, to diagnose asthma, patients will be tested with beta 2 agonists and inhaled corticosteroids with results in reducing clinical symptoms such as relief of dyspnea, reduced lung murmur, peak flow rate. Exhalation is improved.

Lưu lượng kế
2.2 Differential diagnosis Are the symptoms of bronchial asthma similar to some other diseases such as heart attack, pneumothorax and exacerbation of chronic obstructive pulmonary disease, respiratory foreign body, bronchiolitis ,... Some differential diagnoses:
Foreign body in the respiratory tract: showing signs of coughing, shortness of breath, accompanied by cyanosis Heart attack: the patient has a history of heart disease, a history of shortness of breath when Exercise is different from shortness of breath due to bronchial asthma often related to weather, allergic factors. Hear the lungs have moist crackles, more hissing rales, snoring rales. Blood pressure is often very high. In some cases where the distinction is not certain when managing, it is advisable to use beta-agonist spray or vibrating gas, not orally Pneumothorax : No history of dyspnoea, lungs without rales snoring, rales, chest X-ray with pneumothorax in one lung Exacerbation of chronic obstructive pulmonary disease (COPD): History of persistent but not exacerbating dyspnea, dyspnea usually does not begin with small and more common in men who smoke a lot. Bronchiolitis: often accompanied by fever, cough and sputum, and bronchial asthma often has a dry cough.

Một số bệnh lý khác có triệu chứng tương tự hen phế quản
3. Treatment of bronchial asthma
Principles of asthma management include:
Avoiding risk factors for the disease Actively treating flare-ups Treating flare-ups and complications Educating patients about treatment and Long-term follow-up 3.1 Treatment of flare-ups Principles of treatment of flare-ups:
Bronchial smooth muscle relaxants Anti-inflammatory: systemic or local corticosteroids Treat hypoxemia with oxygen, possibly artificial ventilation and other therapies. Other complications if they occur Drugs to treat flare-ups include:
Short-acting b2 adrenergic agonists such as salbutamol, terbutalin, fenoterol, reproterol.pirbuterol. Use orally, injection, spray, aerosol. Possible undesirable effects such as muscle tremors, increased heart rate, increased blood glucose, decreased K + M-choline antagonists: tiotropium bromide, ipratropium bromide, spray or aerosol. Undesirable effects such as thick sputum, difficult to spit, dry mouth, increased heart rate are uncommon,... Methyl xanthin group: diaphylin, theostat, theophylline, used orally or intravenously. May cause gastric mucosal irritation, vomiting, nausea, increased heart rate, even cardiovascular collapse when administered intravenously quickly. However, this group of drugs should not be widely used. During an outbreak, it is necessary to monitor and evaluate the results after 30-60 minutes based on the criteria to assess the severity of the outbreak, respiratory function,...

Sử dụng thuốc điều trị đợt bùng phát
3.2 Long-term treatment Asthma people need long-term treatment to identify and control asthma triggers Prevent chronic symptoms Maintain lung function close to normal Prevent exacerbations Recurrence of flare-ups and minimized hospitalizations and emergencies Medicines used should identify advantages and minimize side effects Educate patient and family on treatment plan Long-term asthma Asthma is a chronic respiratory disease, acute bronchial asthma is an exacerbation of chronic asthma. Therefore, patients need long-term treatment of asthma, when seeing abnormal signs, they should immediately go to a medical facility for timely examination and treatment, to avoid flare-ups of asthma caused by asthma. .
Currently, Vinmec Times City International General Hospital has an Asthma Screening Package to help screen and detect the disease early to promptly control and treat the disease and perform clinical examination, take medical history, measure function respiratory function, ENT examination, bronchial asthma screening.

Định kỳ kiểm tra sức khỏe, giúp mọi người phát hiện bệnh lý sớm
Vinmec Times City's team of highly qualified and experienced doctors; full range of professional means to diagnose, determine the cause of bronchial asthma and stage it before treatment; quick examination time, thorough consultation, easy compliance with treatment management, helping patients feel secure in examination and treatment.
Customers can directly go to Vinmec Health system nationwide to visit or contact the hotline here for support.
MORE:
Asthma Screening Package How to diagnose asthma? Distinguish bronchial asthma and cardiac asthma