This is an automatically translated article.
The article is professionally consulted by Master, Doctor Trinh Thi Phuong Nga - Radiologist - Department of Diagnostic Imaging and Nuclear Medicine - Vinmec Times City International General Hospital.Gastric volvulus is a surgical disease that causes abdominal distension when the stomach is twisted over its intrinsic mesentery. Gastric volvulus if it goes up to 180° and causes bowel obstruction and would be an emergency. Therefore, the rapid diagnosis through early access and recognition of the signs of gastric volvulus on X-ray will help to minimize the damage and improve the outcome for the patient.
1. What is gastric torsion?
Gastric volvulus is a rare clinical entity defined as an abnormal rotation of the stomach with an angle of more than 180°, creating a closed loop of obstruction on the outflow tract of intraluminal fluid into the stomach. in the subsequent gastrointestinal tract. In the majority of cases, gastric volvulus can present as an abdominal emergency or as a chronic problem with intermittent presenting, depending on the degree of torsion and the rate of onset. .Whatever the setting, the classic triad of symptoms associated with gastric torsion includes:
Severe epigastric pain Nausea without vomiting Inability to tolerate food through a nasogastric tube Causes Gastric volvulus is questionable on these hypotheses. For spontaneous gastric volvulus (accounting for 2/3 of cases) the cause is probably due to abnormal laxity of the gastric and duodenal ligaments. For congenital or acquired gastric volvulus, anatomical defects involving the gastric region have been attributed. In the case of a diaphragmatic hernia of the esophagus, the stomach is pulled upwards adjacent to the esophagus, causing the stomach to turn upside down; Therefore, gastric rupture is the most common complication of diaphragmatic hernia. In addition, gastric torsion has also been reported as a surgical complication involving gastro-oesophageal reflux, neuromuscular disorders, and intra-abdominal tumors.
Epidemiology records the same prevalence in men and women. About 10-20% of cases occur in children, usually before 1 year of age. Gastric rupture in children is often secondary to congenital diaphragmatic anomalies. This condition is not common in adults under the age of 50.
Regardless of the cause, in any subject, the prognosis of fatal gastric volvulus without surgery is reported to be up to 80%, due to strangulation, leading to necrosis and ultimately perforation. Later, thanks to advances in diagnosis and treatment, the mortality rate from acute gastric volvulus decreased to 15-20% and chronic to 0-13%.
2. How to approach gastric torsion?
Taking the History The history of the patient with gastric volvulus may present as an acute abdominal condition or as a chronic, episodic problem. Symptoms present depend on the degree of torsion and the rate of onset.For acute gastric torsion, the patient will complain of pain, dyspnea, and inability to tolerate nasogastric tube. The pain is described as sudden onset of severe pain in the epigastrium or left hypochondrium, in the chest, radiating to the left side of the neck, shoulder, arm, and back. Then, the feeling of bloating and slow digestion gradually appeared following the pain. The patient may be distended in the upper abdomen with pain if the stomach is still in the abdomen; However, if the stomach has been pulled up above the ribcage, the symptoms may be less noticeable in the abdomen and easily confused with a heart attack. Occasionally, some patients present with regurgitation secondary to ischemia and mucosal desquamation. Consequences can rapidly progress to hypovolemic shock and hypotension.
For chronic gastric volvulus, patients often present with epigastric pain and bloating after meals. Some patients seek medical attention because of early satiety, shortness of breath, and chest tightness, which may be accompanied by dysphagia if the disease involves the esophagus. However, due to non-specific symptoms, patients are often misdiagnosed with gallstone disease, peptic ulcer disease ... and long-term treatment is not effective.
Examination The findings of gastric examination in patients with gastric torsion may also be nonspecific.
Localized pain and epigastric distension may suggest high intestinal obstruction, including gastric volvulus. In case of severe gastric necrosis or obstruction, peritonitis may occur.
Differential Diagnosis Because the findings on physical examination can be confusing, some of the following common stomach diagnoses are commonly thought of before being attributed to gastric torsion:
Gallstones Myocardial infarction heart Peptic ulcer - duodenal stenosis pyloric stenosis Disc herniation

Xoắn dạ dày là bệnh lý hiếm gặp
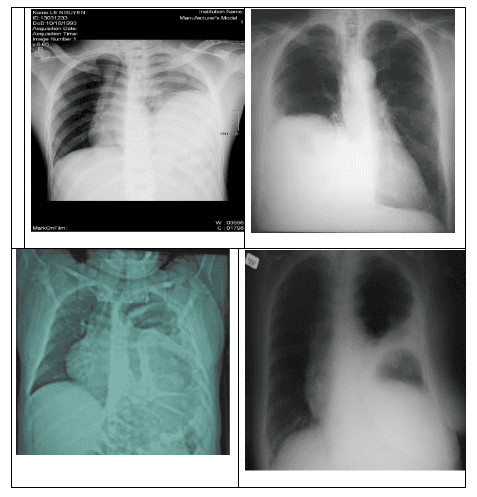
3. Signs of gastric volvulus on X-ray
Indications for radiographic imaging in gastric torsion include straight chest radiographs, unprepared abdominal radiographs, and contrast-enhanced radiographs.Chest X-ray Film On chest x-ray, the sign of gastric volvulus can be seen as the image of gas filling behind the heart balloon in case of stomach herniated diaphragm entering the thorax. This is a sign that confirms the diagnosis.
Abdominal X-ray Abdominal X-ray alone shows a large distended stomach pouch in the upper abdomen.
At this point, the stomach image is oriented horizontally with a single level of water – a single gas level across multiple repeat films. At the same time, the colonic loops are absent.
X-ray film with contrast When giving the patient a contrast agent, the solution will stay in the stomach lumen, showing an abnormal stomach image.
When taking the film again after a period of time, the amount of medicine in the stomach lumen does not change.
4. Other diagnostic means of gastric torsion
Biochemical tests are not usually diagnostic of gastric volvulus; however, increased blood amylase and increased serum alkaline phosphatase (ALP) have also been reported.Besides imaging and radiography, computed tomography also helps confirm the diagnosis with benefits such as rapid image reconstruction, detection of pneumoperitoneum if gastric perforation as well as detection of other weak Associated risk factors such as diaphragmatic hernia and help rule out other abdominal pathologies. At the same time, the findings on the upper gastrointestinal endoscopy may also suggest a gastric tumor, causing gastric torsion.

Chụp cắt lớp vi tính cũng được sử dụng để chẩn đoán xoắn dạ dày
5. How to treat gastric torsion?
Medical Medicines used in the treatment of gastric torsion are primarily aimed at ameliorating the associated symptoms, particularly pain, nausea, and vomiting. Commonly used pain relievers include morphine sulfate and hydromorphone. Commonly used antiemetics include promethazine and ondansetron.Surgery Surgical intervention is the prerequisite treatment for gastric torsion cases, especially emergency surgical repair for acute gastric torsion.
On the other hand, in patients who are not candidates for radical surgery, such as secondary causes after comorbidities, torsion may improve after endoscopic surgery.
In summary, gastric volvulus is a rare abdominal surgical disease. However, with the diagnosis of gastric torsion by x-ray signs and available facilities at each medical center, patients can be detected early and have timely surgery, especially in the acute setting. calculation, limiting serious complications later.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space.
If you have a need for consultation and examination at Vinmec Hospitals under the nationwide health system, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.