This is an automatically translated article.
The article is professionally consulted by Master, Doctor Vo Thien Ngon - Department of General Surgery - Vinmec Da Nang International General Hospital
Urinary TB occurs when the kidneys become infected with TB hematogenously from a TB foci in the lungs, pleura, lymph nodes, or elsewhere. Urinary TB is often detected late after being diagnosed and treated for causes such as urinary tract infections, kidney stones, and kidney cancer.
1. Understanding urinary tuberculosis
Genitourinary tuberculosis ranks second after pulmonary tuberculosis, about 1/6 of pulmonary TB patients have TB in organs other than the lungs such as lymph nodes, intestines, bones, and kidneys. This risk is doubled in patients who are immunocompromised, malnourished or have poor living conditions.
The sex organs (prostate, seminal vesicles, epididymis, fallopian tubes) can also be infected by the way from the kidney or through the bloodstream. The disease appears late, about 5-15 years after primary TB infection, is rare in children and usually affects only one kidney.
2. Symptoms of Urinary TB

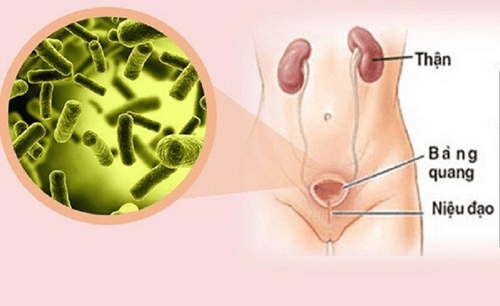
Người bị lao bàng quang thường có hội chứng viêm bàng quang, biểu hiện bằng các triệu chứng rối loạn bài tiết nước tiểu
Symptoms of urinary tuberculosis are often subtle and are first manifested by fatigue, fever in the afternoon, and night sweats. If it is in the bladder, the patient will have cystitis syndrome, dysuria, urinary frequency, sometimes gross hematuria at the end of the field. Clinical examination is usually negative, the renal area may be tender to palpation.
Urinary TB is often detected late after being diagnosed and treated for causes such as urinary tract infections, kidney stones, kidney cancer... However, there are still some common symptoms as follows:
2.1 Urinary excretion disorder Manifested by symptoms of cystitis (60 - 70% in urinary tuberculosis) such as urinary incontinence, especially at night, painful urination at the end of the field. These symptoms are sometimes frequent, sometimes not obvious. The course of the disease usually subsides and then reappears. These symptoms are similar to those of a urinary tract infection.
2.2 Hematuria is a common sign that is usually small in volume, bloody but not painful, or recurrent, often with hematuria, which may be only microscopic hematuria, only identifiable. by urine test.
2.3 Pyuria The patient may have only purulent urine, which is culture negative for common bacteria.
2.4 Low back pain Patients feel heaviness or mild pain in the lower back, sometimes experiencing renal colic due to damage that causes narrowing of the urinary tract, or plaques that move along the urinary tract. cause temporary obstruction, causing ureteral spasm.
2.5 Other symptoms Tuberculosis may be detected in the presence of cystitis, rectal examination sometimes shows tuberculosis spreading to the seminal vesicles and prostate (with solidification areas). If TB is present, the epididymis is enlarged and solid, there may be perineal tuberculous fistulas.
In women who may have adnexitis, infertility, menstrual irregularities and sometimes peritonitis, a thorough clinical examination is necessary to detect extrarenal tuberculosis, especially pulmonary and lymphatic TB. or tuberculosis.
3. Diagnostic tests

Cần thực hiện một số xét nghiệm nhằm chẩn đoán chính xác bệnh
Additional tests needed to diagnose UTI include:
Unprepared abdominal radiograph to show calcifications in the kidney and prostate. Transvenous urography: To show eroded renal papillae, constricted calyces, narrowing, and anterior bulge, narrowing of the ureter can also be seen, often distal. Lesions are more often unilateral than bilateral. Urethrography - retrograde bladder: Shows urethral stricture, with cave in the prostate. Cystoscopy: Visible cystitis lesions or bubble-shaped edema at the entrance of the ureter, in advanced stages, can see tuberculoma, ulceration, and bladder shrinkage due to fibrosis . Renal ultrasound : See lesions in the kidney.
4. Treatment of urinary tuberculosis
The main goals of treatment are to preserve renal parenchyma and function, clear the patient of infection, and control comorbid conditions. Genitourinary TB responds better to a short course of treatment than pulmonary TB because urogenital TB carries a lower amount of TB bacteria. In addition, two key drugs for the treatment of TB, isoniazid (INH) and rifampicin, penetrate well into the cavity-like lesions associated with urinary tuberculosis.
The prognosis for urological tuberculosis that responds well to drug therapy will depend on the extent of the lesion at the time of diagnosis and initiation of treatment. If treated early, kidney tuberculosis and kidney function are not affected.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space.
Doctor Vo Thien Ngon has over 7 years of experience working as a urologist and surgeon at Hospitals: Hue Central Hospital, Hue University of Medicine and Pharmacy Hospital, Tam Tri Da Nang General Hospital .
Doctor Ngon with the ability to specialize in the field of examination and treatment of diseases of the Urology and Andrology system, Urology surgery, endoscopic urological surgery, Laparo urinary tract surgery, endoscopy Urinary. Currently, Dr. Vo Thien Ngon is a Urology - Orthopedic Surgery Doctor, Department of General Surgery, Vinmec Da Nang International Hospital
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.