This is an automatically translated article.
Damage to the brachial plexus occurs during birth causing paralysis or reduced movement and sensation of the brachial muscles. Caused by the rupture or dilation of one or all of the ulnar, radial, and median nerves from the brachial plexus due to the hand and shoulder pulling procedure during delivery.
1. Overview
The median nerve arises from the lateral and medial bundles of the brachial plexus, descends the arm along the brachial artery and then down the forearm, lying between the common flexors of the superficial and deep fingers . Upon reaching the wrist, the median nerve travels down the carpal tunnel to the palmar and branches there.
The median nerve innervates wrist and finger flexion, forearm and table pronation, flexion, abduction, and opposite thumb. In terms of sensation, in the palm of the hand it governs the 1, 2, 3 and 1⁄2 fingers in addition to the 4th finger, in the back of the hand it governs the terminal knuckles of the upper fingers. In addition, the median nerve is a mixed nerve with many sympathetic fibers, so when injured, patients often feel burning pain in the hand.
Damage to the median nerve can be compressed in the wrist region in carpal tunnel syndrome. Carpal tunnel syndrome is the most common cause of peripheral nerve compression. The subjects at risk of carpal tunnel syndrome are people with jobs that require a lot of wrist movement, old age, obesity, diabetes, kidney failure, thyroid dysfunction, osteoporosis. If detected early, carpal tunnel syndrome responds well to conservative treatments. If conservative treatment is not effective, surgery is required. The process of rehabilitation exercise after surgery plays an important role in helping patients recover early and regain hand function.
In addition, the anterior interosseous branch of the median nerve can be compressed in the forearm, causing anterior interosseous nerve syndrome. The median nerve can also be injured at any point in its path from a gunshot or gunshot wound. Depending on the location and extent of the injury, the appropriate treatment, conservative or surgical, is selected. Physical therapy and rehabilitation of damaged median nerve are highly dependent on the treatment chosen.

Hình ảnh điều trị phương pháp vật lý trị liệu
2. Clinical and subclinical diagnosis
2.1. Clinical diagnosis Based on clinical symptoms to diagnose:
Symptoms of soft tissue injury around the shoulder joint Pain: Due to soft tissue hemorrhage Edema: Due to concussion Restriction of passive and active shoulder joint movement due to pain Nerve symptoms: Peripheral flaccid paralysis: Depending on the extent of the injury and the location of the injury, there are different types of paralysis. Radial nerve paralysis: the joints of the fingers and hands lose the ability to extend. Paralysis of the ulnar nerve: When grasping the hand, fingers IV, V and part of the third finger cannot be fully flexed, cannot flex the end of the V toe Paralysis of the median nerve: Monkey hand is when grasping the hand, fingers I and Finger II does not fold Decreased muscle tone: Decreased muscle stiffness Decreased muscle strength Manual muscle test (MMT) to assess paralysis of each muscle group: Grade 0: No minimal muscle contraction. Grade 1: There is muscle contraction during movement. Grade 2: Movement is possible but not full range in the gravity-free position. Grade 3: Exercising full range of motion, with resistance to gravity and moderate or light resistance. Grade 4: Exercising full range of motion, resisting gravity and maximal resistance

Chụp X quang khớp vai
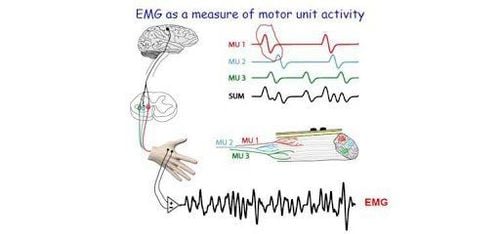
2.1. Subclinical diagnosis Electrodiagnostic survey: electromyography (EMG) and nerve conduction study help identify damaged nerves, localize the damage and help monitor the healing process of nerves Between. Usually, the results of electrodiagnostic investigations are normal in the early stages of the disease.
X-ray: Take a straight shoulder to rule out accompanying bone and joint damage (clavicle fracture, humerus fracture, shoulder dislocation).
MRI: in some cases, MRI helps detect median nerve compression in the forearm, carpal tunnel.
3. Rehabilitation of median nerve damage
3.1. Recovery of median nerve damage in carpal tunnel syndrome Many patients with carpal tunnel syndrome respond well to conservative treatment if detected early. Wear wrist support, keep in neutral position, wear it while sleeping and doing activities that require a lot of wrist movement. Use more oral anti-inflammatory pain relievers. Approximately 90% of patients with mild carpal tunnel syndrome respond to conservative treatment after 4-6 weeks of treatment, followed by maintenance for at least 2 more months.
If the patient has not responded to conservative treatment with a wrist splint, the next option is to inject steroids into the carpal tunnel. Symptoms usually subside after the first injection, in some cases up to 3 injections are allowed, 3-6 weeks apart.
Change position and have a reasonable rest when working to avoid aggravating the disease.
Rehabilitation method:
- Week 1: Exercise immediately after surgery, gently flexing the wrist, flexing and extending the fingers to the maximum. Wear a supportive wrist brace.
- Week 2: Thread trimming and scar care. Start strengthening your muscles and do activities of daily living.
- Week 3-4: Continue strength training. Patient is allowed to do more vigorous activities and return to work

Thuốc giảm đau giúp chống viêm đường uống cho bênh nhân
3.1. Rehabilitation of the median nerve damaged by an injury to the arm or forearm Acute stage: immediately after the injury or after surgery Immobilize the injured limb: the time depends on the condition of the injury and the surgical method. Mobility: the frequency and intensity of exercise also depends on the condition of the injury and the surgical method. Advise the patient on how to safely protect the injured area, especially after neurosurgery. Avoid causing damage to the area of the limb that has lost sensation. Recovery phase: when there are signs of nerve re-innervation Motor retraining: muscle strength training according to the progressive program Decreased hyperesthesia: nerve re-innervation is often accompanied by hyperesthesia sense. Expose the patient to a variety of objects made of different materials to reduce the condition. Sensory retraining: helps the patient learn to recognize objects when touched. Chronic phase: nerve re-innervation has reached its peak, some motor and sensory functions are no longer able to recover.
Vinmec International General Hospital with a system of modern facilities, medical equipment and a team of experts and doctors with many years of experience in neurological examination and treatment, patients can completely peace of mind for examination and treatment at the Hospital.
To register for examination and treatment at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register online HERE.