This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II Pham Thieu Trung - Department of General Surgery - Vinmec Phu Quoc International General Hospital, Specialist Doctor I Tran Thi Anh Hien - Department of Surgical Anesthesia - Hospital Vinmec Central Park International General Hospital.Spinal anaesthesia, also known as subdural anesthesia, is an effective, highly reliable, relatively simple anesthesia method, with few complications and complications, but it is necessary to respect basic principles such as aseptic , drugs with absolute purity, small needles and especially attentive patient care. Frequently asked questions from patients such as what complications from spinal anesthesia or whether spinal anesthesia cause back pain will be answered below.
1. What is spinal anesthesia?
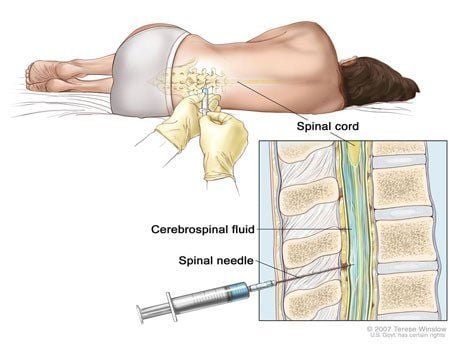
Spinal anesthesia, precisely called subarachnoid space anesthesia, is a method of regional anesthesia that is performed by introducing an appropriate amount of local anesthetic into the subarachnoid space, causing the anesthetic to mix with the cerebrospinal fluid. The initial local anesthetic has a large concentration, but when mixed with the cerebrospinal fluid, the concentration is smaller than the initial concentration and affects the nerve roots, causing loss of sensation and motor paralysis. This is a special numbing method in the field of anesthesia and resuscitation, so only those who have a lot of experience and master the principles should do it.

Gây tê tủy sống được thực hiện tại cơ sở y tế uy tín
2. Mechanism of action of local anesthetics in spinal anesthesia
When local anesthetic is injected under the dura, the anesthetic will penetrate the spinal nerve roots and sympathetic branches above and below the needle puncture area, from the spinal cord to the outside, through the subdural space. has the effect of cutting off the transmission of nerve impulses, causing rapid paralysis of the sensory, motor and sympathetic nerves that control both lower extremities, abdominal wall and internal organs. belly.
Some factors affect the spread of drug anesthesia include:
Injection site Patient position Patient dosage Dose of injected drug Volume injected The speed and force of anesthetic injection Duration of action depends on each patient. type of local anesthetic Specific gravity of local anesthetic

Vị trí gây tê ảnh hưởng đến cơ chế tác dụng của thuốc tê
3. How is spinal anesthesia performed?
Before spinal anesthesia, it is necessary to comprehensively examine the patient to review and evaluate the patient's condition and explain to the patient clearly. The night before surgery, give the patient a sedative.
Posture for lumbar puncture includes:
Sitting position: Easy to do because the intervertebrae are dilated but not used when the hemodynamic status is unstable. Prone position: The most difficult to puncture, so it is only used when operating in the prone position and the patient cannot lie in other positions. Side-lying position: The most commonly used and applicable to all methods of spinal anesthesia. The patient lies on his side, with the shrimp's back arched, the spine parallel to the operating table, the shoulders and two pelvic spines perpendicular to the operating table, the thighs folded in front of the abdomen, the head and neck bent forward. Lumbar puncture can be midline, lateral line, or lateral lumbar line. The location of the puncture is the horizontal line of the two iliac crests passing through the middle of the lumbar segment 4-5 from there, counting up or down depending on the requirements of the puncture site. The probing procedure is as follows:

Gây tê tủy sống dưới sự hỗ trợ của máy siêu âm
Use local anesthetic such as lidocaine 1% 1-2 ml local anesthetic in the skin or under the skin. Insert the needle into the space between the two posterior vertebrae, pushing the needle inward from the outside to the inside. Push the needle slowly in, so that the bevel side of the needle is horizontal, when it is 4-5 cm deep, the needle will touch the solid, solid tissue of the yellow ligament. dura and into the subdural space. At this time, there will be a feeling that there is no more resistance. When you pull out the pine tree, you will see that the cerebrospinal fluid is as clear as spring water. When there is no blood in the cerebrospinal fluid, attach the syringe containing the anesthetic to the pin. Pump gently and slowly about 1-2 ml over 2-3 minutes. If you want to increase the level of anesthesia, you can use a pump, withdraw a little cerebrospinal fluid to mix the anesthetic solution and then continue to pump it in and repeat it a few times. After the injection of local anesthetic is complete, withdraw the lumbar puncture needle, disinfect the puncture site, apply a sterile dressing, and position the patient as required by surgery. Monitor the patient's vital signs closely, continuously and manage possible complications and monitor the high and low level of numbness.
4. Complications of spinal anesthesia
Spinal anesthesia can cause complications and complications such as:
Headache: A common complication after spinal anesthesia because cerebrospinal fluid escapes through the puncture hole. Headaches vary by position, pain in the top and sides of the temples, lying down or keeping the head low will relieve the pain. Headache will resolve on its own after an average of a few days, to minimize complications need to use as small a needle as possible medication
Back pain : Not more than after anesthesia if the midline lumbar puncture is accurate, does not cause damage Injury to the adjacent organs of the spine.
Low blood pressure: Common after 20 to 30 minutes of spinal anesthesia due to parasympathetic nerve paralysis, causing vasodilation in the numbed area, keeping blood in the periphery. Mild reductions in blood pressure with spinal anesthesia do not require intervention, but if severe, prompt fluid resuscitation, leg elevation, oxygenation, and intravenous atropine should be given if bradycardia is present.
Respiratory reduction: In fact, spinal anesthesia does not affect respiratory function, respiration only decreases when the level of anesthesia is too high, partially paralying the intercostal muscles or diaphragm, seen in the influence of the morphine group. such as morphine, dolosal,...
Vomiting: Due to spinal anesthesia, blood pressure is reduced, causing cerebral hypoxia.
Urinary retention : Seen after surgery because the nervous system controlling urination has not been fully restored, which usually disappears after a few days.

Người bệnh xuất hiện triệu chứng đau lưng
Infection : Usually due to unsanitary principles, sterile instruments.
Neurologic sequelae: very rare, such as VI nerve palsy, cauda equina or meningeal thickening, radiculitis.
Graduating from the residency training program, Dr. Tran Thi Anh Hien has experienced many different working environments such as Binh Dan Hospital, Ho Chi Minh City University of Medicine and Pharmacy Hospital and French-Vietnamese Hospital. before returning to work at the Anesthesia and Anesthesia Unit - Department of Surgical Anesthesia - Vinmec Central Park International General Hospital.
To learn more, you can contact Vinmec Health System nationwide, or register online HERE
Recommended video:
Spinal plane anesthesia (ESP): Complete pain relief, no need for morphine
MORE:
Intraoperative spinal anesthesia: Indications and contraindications Some complications, side effects of spinal anesthesia in surgery Differentiate epidural and spinal anesthesia