This is an automatically translated article.
Minimal pleural drainage or minimal pleural effusion is indicated for the purpose of removing fluid or air from the pleural space by placing a pleural tube through the chest wall.
1. Why minimal drainage of the pleural space is required?
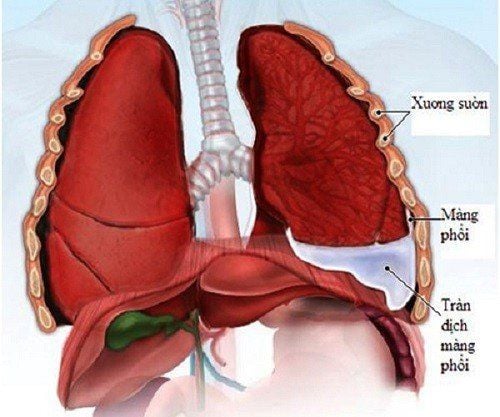
Normally the pleural space is a virtual space created by the parietal and visceral pleura. Normal pleural pressure is a negative pressure of about -2 to -4 mmHg, which varies with inspiration and expiration. For some reason, there is fluid, gas, blood, ... in the pleural cavity, which changes the negative pressure in the pleural space, affecting the respiratory function. The lungs cannot perform the function of supplying oxygen to the whole body, leading to shortness of breath and even respiratory failure. Therefore, minimally pleural effusion is a procedure to free the pleural space from pressure by air or fluid, and return the pleural space to its original state as a negative-pressure virtual space by placing a drainage tube. through the chest wall.
2. Indications for minimal pleurodesis
Pneumothorax : Massive pneumothorax Pneumothorax in a patient with unstable clinical symptoms Tension pneumothorax Recurrent pneumothorax Traumatic pneumothorax lung due to the physician's procedures into the pleural space such as tumor biopsy, pleural effusion. Hemothorax after trauma or procedure Esophageal fistula pleural effusion Cancer pleural effusion Rapidly recurring pleural effusion Causing pleural adhesions through drain tube Empyema Esophageal fistula pleural effusion Pleural drainage minimally after thoracic surgery.
Chỉ định mở màng phổi tối thiểu đối với bệnh nhân tràn khí màng phổi
Trắc nghiệm: Làm thế nào để có một lá phổi khỏe mạnh?
Để nhận biết phổi của bạn có thật sự khỏe mạnh hay không và làm cách nào để có một lá phổi khỏe mạnh, bạn có thể thực hiện bài trắc nghiệm sau đây.3. Contraindications
There are no absolute contraindications.
Relative contraindications to pleural drainage:
Coagulation disorders, hemostasis: prothrombin ratio <50% and/or platelet count <50G/l. Hemodynamic disorders. Injury to the skin of the chest wall in the area where the pleural opening is planned.
4. Implementation process
The process must ensure four principles: sealed, aseptic, one-way and continuous suction with control pressure > -20cm H2O and < -30 cm H2O.
Determine the location of drainage: Based on computed tomography film, or chest X-ray film to choose the patient's position when conducting the procedure. Perform pleural effusion: Disinfect the drainage area Anesthetize the area of the pleural opening. Anesthetize the chest wall in layers, from the skin to the parietal pleura. Using an anesthetic needle to probe the pleural space Skin incision and fascia are made along the intercostal space along the superior border of the ribs to avoid injury to the intercostal nerve bundle. The incision is wide enough to allow the drainage tube to be inserted. Use a trowel to separate each layer of chest wall muscle along the muscle fibers until the parietal leaf, then use a pin to puncture the pleural space Insert the drain into the pleural space through the hole just opened. For pneumothorax, the direction of the drain is anterior and apical, and for pleural effusion, the direction of the tube is posterior and downward Fixing the drain Connect the other end of the drain to Vacuum cleaner with suction pressure -20cm H2O.
5. Attention during drainage placement
After the drain is connected to the suction system with the appropriate pressure, aspirate all the fluid and calculate the hourly discharge. If there is no drainage from the drainage, check if the drainage is clear. If the column of fluid in the drain tube fluctuates with the patient's breathing, it means that the drainage tube is still open and the fluid has been exhausted. Check whether the lungs are enlarged after drainage by: Clinical examination to assess the patient's condition, check the lungs.
6. Some complications may occur in minimally drained pleural space surgery
Chest pain. Bleeding from puncture of the intercostal nerve bundle: surgical intervention if necessary.

Bệnh nhân có thể thấy đau ngực trong phẫu thuật dẫn lưu tối thiểu khoang màng phổi
Wrongly poke into the adjacent organs (lungs, liver, spleen, stomach,...) to avoid needing to master the anatomical position, determine the exact position of pleural opening based on X-ray film, Computed tomography of the chest, ultrasonography of the pleural cavity. Fainting due to fear: this is a common complication. Acute pulmonary edema: can occur when aspiration is high pressure, fluid is released too quickly and a lot. Infection due to non-compliance with aseptic rules during the procedure. To register for examination and treatment at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register online HERE.