This is an automatically translated article.
The article was professionally consulted by Doctor Vo Ha Bang Suong - Doctor of Medicine - Department of Medical Examination & Internal Medicine - Vinmec Phu Quoc International General Hospital. The doctor has more than 15 years of experience in the treatment of internal diseases.Aspergillosis is an opportunistic infection caused by inhaling the spores of the fungus Aspergillus. It is a type of plant parasite. In the body, Aspergillus is saprophytic (endogenous, exogenous), they cause disease when the body has favorable conditions such as using many antibiotics, using corticosteroids for a long time to disturb the balance between bacteria and fungi. saprophytic and fungal growth, or immunocompromised body such as HIV/AIDS, organ transplant. Diagnosis is mainly based on clinical, can combine with laboratory tests such as culture, histopathology, imaging support. There are many types of Aspergillus fungi, such as A. fumigates, A. flasus, A. Niger, A. nidulans; however, only a few species causing human disease have been found, mainly A. fumigates, rarely other species.
1. Favorable conditions for Aspergillus infection
Immunocompromised: People who take immunosuppressive drugs after undergoing transplant surgery, especially bone marrow or stem cell transplants, or those with certain blood cancers are at increased risk for aspergillosis. highest penetration. People in the later stages of AIDS may also be at risk for this fungus (Aspergillus, however, is less common in HIV/AIDS patients). Low white blood cell levels. People who have received chemotherapy, organ transplants, or leukemia have lower levels of white blood cells, making them more susceptible to invasive aspergillosis. Prolonged corticosteroid therapy. Depending on the condition being treated with corticosteroids and other medications being used, prolonged use of corticosteroids may increase the risk of aspergillosis and similar infections. Organ transplant (especially bone marrow transplant).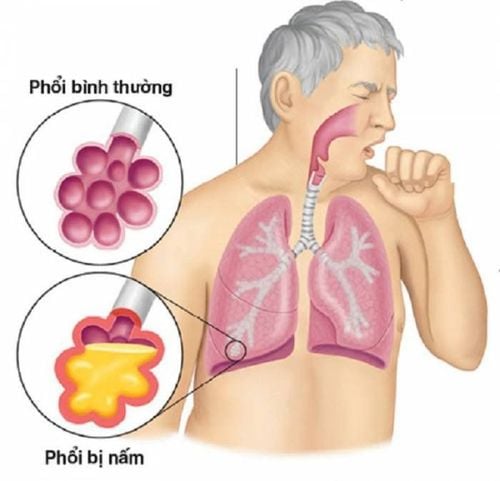
Nhiễm trùng nấm Aspergilloma ở phổi
2. Aspergillus infections
Invasive infections are usually caused by inhalation of fungal spores, sometimes by direct invasion through damaged skinAspergillus sp has a tendency to infect empty spaces, eg caverns created by previous lung disease (eg, bronchiectasis, lung tumor, tuberculosis), infection of the sinuses or external ducts (fungal ear infection). This infection is usually invasive and destructive at the site of injury, but can occasionally progress to progressive disseminated infection, particularly in immunocompromised patients with leukopenia or corticosteroid use. However, aspergillosis is uncommon in HIV-infected patients.
fumigatus is the most common cause of invasive lung disease; A. flavus often causes extrapulmonary invasion, possibly because these patients are more immunocompromised than A. fumigatus-infected patients.
Lung mycoma : Localized infection, typically in the lung, sometimes forming an aspergilloma, characterized by a large mass of mycelium, fibrin, and a small number of inflammatory cells, covered externally by fibrous tissue. Occasionally, there are cases of tissue invasion outside the cavity, but usually the fungus is confined to the cavity without significant external invasion.
Chronic invasive aspergillosis may occur, especially in patients receiving long-term corticosteroids, and chronic granulomatous disease is characterized by inherited phagocytic cell defects.
Aspergillus sp can also cause endophthalmitis following trauma or surgery to the eye or hematogenously and can infect the endothelium causing disease
Primary superficial aspergillosis is uncommon but can occur in burn; under the wound dressing; after trauma to the cornea (keratitis ); or in the sinuses, mouth, nose, or ear canal.
Allergic bronchopulmonary Aspergillus infection: is a hypersensitivity reaction to A. fumigatus leading to pneumonia unrelated to tissue invasion.

Nhiễm trùng nấm Aspergilloma có thể xâm chiếm khu vực xoang
3. Clinical symptoms
Signs and symptoms vary with the type of disease to which a person responds to aspergillosis:3.1. There are many forms of Aspergillus fungal diseases such as bronchi, Aspergillus cysts in the lung remnants, Allergic bronchial Aspergillus, invasive pulmonary Aspergillus. In immunocompromised people with AIDS, when fungal infections of the blood, spread to the lungs are considered opportunistic infections.
3.1.1 Bronchial form Often inflammation in the large bronchi, bronchial mucosa is scratched and then develops a layer of Aspergillus fungus.
+ Allergic bronchopulmonary Aspergillus disease (Hinson's disease): Patients often have recurrent fever, cough with thick sputum, fungal mycelium, and wheezing, such as asthma. More common in that location has bronchial asthma.
3.1.2. Infiltrative form Is a fungal infection of the lungs that then spreads through the bronchial wall into the peripheral alveoli, necrotic lesions and spread by Aspergillus invading the lung parenchyma and blood vessels. The disease is common in patients with acute leukemia and prolonged chemotherapy.
Clinical: Patients often have high fever, cough with difficulty breathing, and hemoptysis occurs in about 50% of patients.
3.1.3. Aspergillus tumor in lung cavity This is a fungal tumor that develops on the new squamous epithelium of a cavity in the lung parenchyma such as cavernous tuberculosis, cavernous abscess. Between Aspergillus and bacteria that cannot reproduce and grow at the same time, the fungus secretes antibiotics. But when the Aspergillus fungus dies, superinfection can appear.
Clinical: Coughing up blood is a common symptom, in patients with fibrous lesions in the lungs who have repeated hemoptysis, Aspergillus tumor should be considered.
3.1.4. Chronic pulmonary aspergillosis May have mild, painless symptoms despite the disease
3.2 Invasive fungal infection extrapulmonary Occurs in severely immunocompromised patients. The disease begins with skin lesions, sinusitis, or pneumonia and may involve the liver, kidneys, brain, and other tissues; often causes rapid death.
3.3 Aspergilosis in the sinuses In the sinuses, fungal infections or allergic sinus infections or chronic invasive granulomatosis can develop with fever, rhinitis, and headache. Patients may have necrotic skin lesions on the nose or sinuses, palatal ulcers or gingivitis, signs of cavernous sinus thrombosis or pulmonary or diffuse lesions.
Aspergillus cysts are usually asymptomatic, although mild cough and occasional hemoptysis may occur.
4. Subclinical
4.1 Diagnostic imaging Chest X-ray is indicated; however, chest CT is more sensitive and should be indicated in high-risk patients (neutropenia). CT sinus is indicated if fungal sinus infection is suspected. Cavernous migratory fungal balls are characteristic lesions that can be detected in both, although most lesions are solid and localized. Occasionally, a halo around a nodule or a cavernous appearance can be seen in a necrotic lesion. Diffuse interstitial pneumonia has been observed in some patients.4.2. Culture and histology of the lesion are necessary to confirm the diagnosis; Histopathology helps to distinguish invasive infections from isolated but nonpathogenic lesions. Lung specimens are usually obtained through bronchoscopy or percutaneous biopsies; Sinus specimens were obtained through otolaryngoscopy. Because cultures take time and histopathology results can be falsely negative, most treatment decisions are based on sound clinical evidence. In Aspergillus endocarditis, large fungal fragments often release large amounts of embolism and provide diagnostic specimens.
4.3. Galactomannan antigen test Galactomannan antigen test in serum and bronchoalveolar lavage fluid.
Antigen tests such as galactomannan are specific, but have low serological sensitivity to identify the majority of cases in the early stages of the disease In invasive pulmonary aspergillosis, the galactomannan test in bronchoalveolar lavage It is much more sensitive than serum and is often the only option for patients with thrombocytopenia because it is not diagnosed by biopsy. Blood cultures are almost always negative, even in rare cases of endocarditis.
4.4. Other supporting tests Blood count leukocytes are not increased and eosinophils percentage is increased
Diagnosis is mainly clinical
Người mắc bệnh hen suyễn nguy cơ cao phản ứng dị ứng với nấm mốc aspergillus
5. Complications
Depending on the type of infection, aspergillosis can cause a range of serious complications such as:Respiratory failure due to heavy bleeding in the lungs Systemic infections. The most serious complication of invasive aspergillosis is the spread of the infection to other parts of the body, especially the brain, heart, and kidneys, and can be fatal.
6. Treatment
6.1 Antifungal drugs Depending on the type of disease and the individual patient to choose the right antifungal drug. Possible antifungal drugs: Voriconazole, Isavuconazole. Amphotericin B (including lipid formulation), Echinocandins as salvage therapyInvasive infections requiring intensive treatment with voriconazole or isavuconazole - drugs with similar efficacy to voiriconazole and with fewer side effects.. Amphotericin B (especially lipid formulations) are also effective, although more toxic. Oral posaconazole or itraconazole (but not fluconazole) may be effective in some cases. Caspofungin or other echinocandins may be used as salvage therapy. Combination therapy of Voriconazole and Echinocandins is effective in certain patients.
Usually, complete recovery requires cessation of immunosuppression (eg, resolution of neutropenia, cessation of corticosteroids). Relapse is common if agranulocytosis continues.
6.2 Surgery Aspergillus infections do not require treatment nor respond to systemic antifungal therapy but may require surgical excision because of local consequences, especially hemoptysis.
7. Prevention
It's nearly impossible to avoid exposure to the mold aspergillosis, but if you've had a transplant or are undergoing chemotherapy, try to stay away from places where you might encounter mold, such as construction sites. construction, composting and grain storage. If your immune system is weakened, your doctor may recommend wearing a mask to avoid exposure to aspergillus and other airborne infectious agents.Prophylaxis with posaconazole or itraconazole may be considered for high-risk patients (those with graft-versus-host disease or leukopenia due to acute myeloid leukemia).
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
Article referenced source: Mayoclinic.org