This is an automatically translated article.
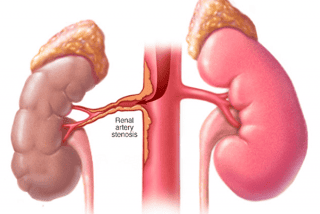
Renal artery stenosis is caused by many different causes. The two most common forms of renal artery stenosis are: fibromuscular dysplasia and atherosclerosis. Renal artery stenosis, if not detected early and treated promptly, will cause dangerous complications.1. Renal artery stenosis
Renal artery disease includes lesions affecting the renal arteries, which can be large, or small or medium sized. The disease can be primary (congenital damage) or secondary to another disorder. The course of the disease can be acute or chronic. The main clinical manifestation of this disease is hypertension.2. Symptoms of renal artery stenosis
Renal artery stenosis, if not detected early and treated promptly, will cause dangerous complications such as:Malignant hypertension, sudden increase in blood pressure, uncontrolled by conventional treatments. often lead to stroke. Decreased renal parenchymal perfusion leads to chronic renal ischemia, which can lead to renal atrophy. One study reported that 14-49% of patients had renal atrophy at the time of diagnosis of renal artery stenosis. Progressive renal failure: Chronic renal ischemia leads to atrophy of the glomerular complexes. If the patient progresses to end-stage renal failure, requiring dialysis, the mortality rate is 30% and the median survival time of patients with renal artery stenosis is 27 months.

Hẹp động mạch thận có thể gây tăng huyết áp ác tính nếu không được phát hiện sớm và điều trị kịp thời
3. Indications and contraindications for renal artery intervention
Indications of percutaneous renal artery intervention include:Renal artery stenosis causing malignant hypertension, hypertension not controlled by medication. Renal artery stenosis causes progressive renal failure. Renal artery stenosis in a patient with one kidney. Renal artery stenosis causes recurrent symptoms of heart failure or transient pulmonary edema. Symptomatic improvement in patients with renal artery stenosis and concomitant unstable angina or heart failure. Along with that, there are also contraindications for
Renal artery stenosis that is not much and has not yet caused symptoms. Progressive infectious diseases, coagulation disorders, uncontrolled renal failure... Renal artery stenosis accompanied by other complicated diseases...
4.Steps to proceed
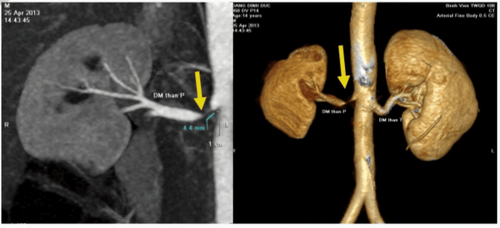
4.1. Vascular access Opens access to the radial or femoral artery. Usually the femoral artery access route is used. In some cases (renal artery origin from top to bottom or aortic or iliac artery disease) can use the radial artery or brachial artery. Set sheath 6F, 7F, or 8F, as appropriate. Once the vascular access is opened, take anticoagulant (heparin) and maintain the ACT at 250-300 seconds. 4.2. Aortic angiography Abdominal angiography allows to assess the location of the renal artery orifice, the presence of renal artery stenosis, the presence of an accessory renal artery, and the degree of aortic calcification.4.3. Interventional Catheterization Connect the catheter to a Y-lock system, manifold. Before inserting the catheter through the arterial sheath, flush the fluid several times to ensure there is no air in the guiding-manifold-contrast injection system. Place an interventional catheter into the renal artery lumen. Connect the tail guiding catheter to the manometer line. A peak-to-peak pressure difference of > 20 mmHg is considered to have limited renal outflow. 4.4 Carrying out renal artery intervention Insert the intervention guidewire through the injured site, after the guidewire tip has passed the injury, continue to push the guidewire to the distal end of the renal artery. 0.014 inch, 0.018 inch, or 0.035 inch guidewire can be used. The 0.014 inch guidewire is preferred because most devices such as stents, balloons, etc. are best suited to the 0.014 inch guidewire. Avoid using hydrated guidewires and rigid guidewires because of the risk of perforating the lateral renal artery and causing bleeding. Conduct balloon angioplasty to widen the lumen of the lesion site. The average ball size is 3.4 to 5 mm in diameter, 8 to 15 mm in length. If the renal vessels are narrow and the atherosclerosis is severe, a smaller balloon may be needed. Renal artery stenting. In the case of fibromuscular dysplasia, balloon dilatation alone is sufficient. However, if renal artery stenosis is due to atherosclerosis, the patient usually needs a stent. Balloon stents are often used instead of self-expanding stents, especially when interventional foramen or proximal renal arteries are performed. Stent diameter ranges from 5-8 mm, length 10-20 mm. After stenting, it may be necessary to re-expand with a high-pressure balloon to ensure complete expansion of the stent. In the case of renal artery stenosis, the stent should cover the entire lesion, and protrude about 1 to 2 mm into the abdominal aorta. In the case of atherosclerosis causing bilateral renal artery stenosis, the doctor can choose to intervene both at the same time or in two phases. Renal artery angiogram after intervention: assess whether there is distal embolism, renal vessel perforation, or renal parenchymal bleeding. 4.5.Patients care after the procedure

Sau khi tiến hành thủ thuật cần theo dõi sát số đo huyết áp của bệnh nhân
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.