This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
Crohn's disease is a form of inflammatory bowel disease IBD (Inflammatory Bowel Disease) causes inflammation, penetrates the wall of the digestive tract causing ulcers, bleeding.
The disease occurs at all ages, but the highest rate is young people. The disease causes a lot of trouble for the patient, if not detected and treated can cause dangerous complications.
1. Causes of Crohn's Disease
To date has not been determined with certainty, but damage to the immune system affects the ability of antibodies (ability to make antibodies) against pathogens and genetic factors (due to genetic mutation) is of interest to many scientists. In addition, pathogens such as pathogenic microorganisms (bacteria, viruses, parasites), improper diet are also pathogens of concern. In addition, some factors favor the occurrence or worsening of Crohn's disease such as smoking, genetics, living in an environment with the influence of dust, chemicals (industry, laboratory). . is also mentioned.
For effective treatment, it is best to determine the cause and extent and location of the lesion, and on the basis of the determined results, the examining doctor will have a specific treatment direction for each patient (using it). medication or surgery). To do that, when you see a prolonged digestive disorder (abdominal pain, loose stools, blood, nausea, vomiting...) accompanied by fever, you need to see a doctor, preferably a gastroenterologist. Patients should not self-diagnose their disease and should not buy drugs for treatment without medical expertise, especially based on the advice of some unqualified drug sellers (just for the profit of the patient). them) will make the disease not only not cured but also aggravated and dangerous.
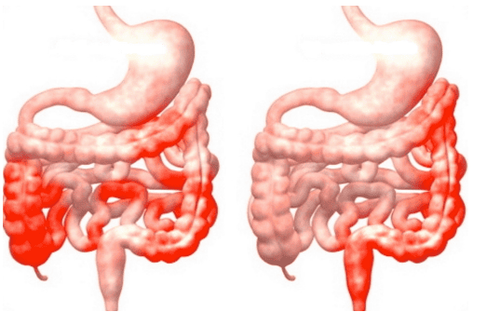
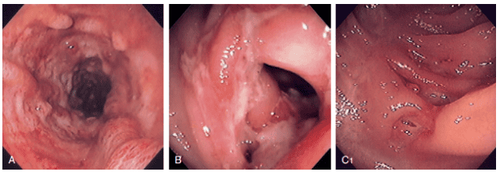
Đặc điểm tổn thương của bệnh Crohn là tổn thương từng đoạn không liên tục trên ống tiêu hoá
2. Clinical Manifestations of Crohn's Disease
Clinical manifestations of Crohn's disease are quite diverse and vary between patients depending on the location and extent of the lesion, age of onset, gastrointestinal complications, and extra-gastrointestinal manifestations. Symptoms and signs of Crohn's disease can sometimes be sudden and very severe. In the majority of cases, the initial symptoms are mild and nonspecific, which can lead to delayed diagnosis.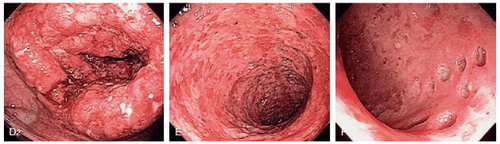
Hình ảnh nội soi của bệnh Crohn
3. Manifestations of gastrointestinal damage
Gastrointestinal symptoms in Crohn's depend on the location, extent, and activity of the disease at the time of diagnosis. Patients with small bowel lesions often present with abdominal pain while patients with colonic lesions often have diarrhea, bloody stools, and dull abdominal pain. Classification of patients according to the location of the lesion helps to assess the severity and predict the cases at risk of surgery or recurrence.
Lesions in the ileum - colon Approximately 50% of patients have lesions in both the terminal ileum and the right colon. Clinically, up to 2/3 of patients have right lower quadrant abdominal pain. If there is partial obstruction of the intestinal lumen due to the narrowing lesion, the patient may have postprandial pain for 30 to 60 minutes.
Symptoms with a lower frequency include blood fractions (22%), malabsorption syndromes such as weight loss, muscle atrophy (12%). Approximately 20% of patients have lesions in the ileum-colon and also have perianal fistula lesions. Extra-gastrointestinal lesions were less common in this group than in patients with colonic lesions alone, but the rate required surgery was higher. A cohort study conducted at the Cleveland Clinic in the US reported that up to 91.5% of patients with both ileocolonic lesions had to undergo at least one surgery at the terminal ileum and colon. right colon or both. Among them, the indications for surgery include intestinal obstruction, intestinal perforation, abscess formation, toxic colonic dilatation, and anal fistula. The study found no difference in 10-year survival in this group of patients.
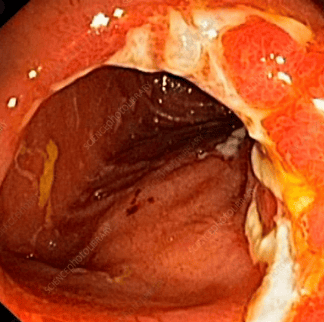
Tổn thương của bệnh Crohn ở đại tràng được nhìn thấy qua nội soi đại tràng
Simple ileal injury This is the second most common type of lesion, accounting for 30% of patients. Patients may have severe, sudden, or insidious onset of symptoms. Cases of progressive ileitis may present with nausea, loose stools, weight loss, low-grade fever, sometimes presenting with acute right iliac fossa pain that can be confused with appendicitis. Diarrhea can range in severity from mild to severe, both during the day and at night, with or without meals, but after large meals, the patient may experience more pain. Symptoms related to anal fistula or bloody stools were less common than in patients with colonic lesions. Colonic involvement Approximately 20% of patients with Crohn's disease have isolated colonic involvement and are sometimes difficult to distinguish from hemorrhagic ulcerative colitis. Lesions are usually concentrated in the right colon and may extend to the entire colon. This group of patients often has rectal bleeding, anal fistula complications and a higher rate of extra-gastrointestinal manifestations (skin lesions, joints...) are higher. According to a longitudinal follow-up study, 24% of patients in this group later developed small bowel lesions and the 10-year surgical rate was approximately 50%.
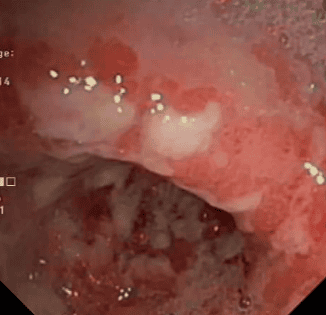
Hình ảnh bệnh Crohn ở hồi tràng được nhìn thấy qua nội soi với nhiều ổ loét
4. Perianal Crohn's disease
According to studies, the proportion of Crohn's patients with associated perianal diseases ranges from 22-45% with an average progression time from diagnosis of 4 years and common in the group with colonic lesions. The most common complications are fistula, ulcer, abscess, stricture with diverse symptoms including pain, bleeding from the anus, bowel incontinence and greatly affect the quality of life of patients. Perianal diseases can be divided into three groups: skin lesions (anal folds, prolapsed hemorrhoids), anal canal lesions (fissures, ulcers, narrowing of the anal canal) and perianal fistulas.
Tổn thương nhiều lỗ rò ở hậu môn do bệnh Crohn
5. Classification of perianal diseases in Crohn's
a. Skin folds There are two types:Large, edematous, hard, possibly bluish-violet skin folds, often arising from fissures or anal sores after healing. Cutting is contraindicated in these skin folds due to the difficulty of wound healing. Excess skin folds form "elephant ear" with flat, flat, painless features. Patient has difficulty in hygiene. This type of excess skin can be safely cut. b. Prolapsed hemorrhoids: Internal hemorrhoids can prolapse but are not common
c. Anal fissures or lacerations: Wide, deep, difficult to demarcate and may be accompanied by an excess skin fold at the edge. Often there are multiple fissures and the patient does not feel pain. If the patient is in pain, an acute inflammatory or abscessed lesion should be suspected on the background of an old fissure Anal ulcer: Usually occurs when there is proctitis, stricture, fistula or abscess formation in the anorectal region
d. Anal fistula : Usually occurs when there is proctitis, stricture, fistula or abscess formation in the anorectal area
e. Recto-vaginal fistula: Fistula lesions on the surface, intersphincter, transsphincter, on the sphincter or outside the sphincter create a connection between the anal canal, rectum and vagina f. Perianal abscess: The soft tissue around the anus is infected with the anus, creating an abscess, which can be around the anal canal, the intersphincter or above g. anorectal stenosis: Due to edema, congestion or deep ulcers in the anorectal region, narrowing h. Carcinoma: On the background of chronic fistulas or ulcers, can progress to malignant lesions: squamous cell carcinoma, basal cell carcinoma or adenocarcinoma
6. Injury to the upper gastrointestinal tract
Usually uncommon in Crohn's. Wagtmans et al.'s study on 940 patients recorded 72 cases, accounting for 8%, with diseases of the mouth, esophagus, duodenum, and jejunum accompanied by upper gastrointestinal tract manifestations. Nugent and Roy proposed criteria for the diagnosis of duodenal ulcer in Crohn's including:Histopathological presence of granulomatous inflammatory lesion formation in the duodenum, with or without evidence of Crohn's in the locality. elsewhere in the gastrointestinal tract. There is evidence of Crohn's disease elsewhere in the gastrointestinal tract and on imaging/endoscopic imaging, diffuse inflammation in the colon is consistent with the Crohn's. This criterion is then also applied to lesions in the esophagus, stomach, and jejunum. Approximately one-third of patients with upper gastrointestinal tract lesions at baseline do not have a confirmed Crohn's diagnosis. The clinical manifestations of this group of patients are usually epigastric abdominal pain, bloating, nausea, fatigue, weight loss and these symptoms are often atypical. Esophageal injury is quite rare (less than 2%) with symptoms such as dysphagia, painful swallowing, retrosternal pain, burning. Stomach injury reported by Wagtman et al. is also very low (0.5%) with Endoscopic findings are similar to those of H. pylori gastritis, and gastric pain is the predominant symptom. Injury to the duodenum accounts for 1 - 7% of patients with newly diagnosed Crohn's, in which the duodenal bulb and duodenum are common. In some reports, the rate of jejunal lesions was found in 4-7% of Crohn's patients and was detected mainly by techniques such as capsule endoscopy, double-balloon small bowel endoscopy, computed tomography. computer ... Cases of diffuse jejunitis - ileum are common in children and adolescents, characterized by ulcers and narrowing in many locations of the small intestine. This condition can lead to small intestinal bacterial overgrowth and intestinal protein loss. The incidence of lesions in the oropharynx and oral cavity ranges from 4 to 12% including oral mucositis, aphthous ulcers, lip swelling, granulomatous lesions. In children and adolescents, Menkersson - Rosenthal syndrome with congenital granulomatous lesions of the mouth or maxillofacial region may be present with recurrent facial paralysis.
Tổn thương ở hang vị dạ dày do bệnh Crohn
Vinmec International General Hospital is a prestigious address trusted by many patients in performing diagnostic techniques for digestive diseases, diseases that cause chronic diarrhea, Crohn's disease... Along with that, at Vinmec Hospital, screening for gastric cancer and gastric polyps is done through gastroscopy with Olympus CV 190 endoscope, with NBI (Narrow Banding Imaging) function for The imaging results of mucosal pathology analysis are clearer than conventional endoscopy, detecting ulcerative colitis lesions, early gastrointestinal cancer lesions... Vinmec Hospital with facilities With modern quality and equipment and a team of experienced experts, always dedicated to medical examination and treatment, customers can rest assured with gastroscopy and esophagogastroduodenoscopy at Vinmec International General Hospital. .
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References
Dao Van Long, Dao Viet Hang. Autoimmune allergic disease of the gastrointestinal tract. Medical Publisher. Bernstein C. N. and Shanahan F. (2008). Disorders of a modern lifestyle: reconciling the epidemiology of inflammatory bowel diseases. Gut,57(9), 1185 - 1191. Nell S., Suerbaum S., and Josenhans C. (2010). The impact of the microbiota on the pathogenesis of IBD: lessons from mouse infection models. Nat Rev Microbiol, 8(8),564-577. Binder V. (1998). Genetic epidemiology in inflammatory bowel disease. Dig Dis Basel Switz, 16(6), 351-355. Montgomery S. M., Morris D. L., Pounder R. E. et al (1999). Asian ethnic origin and the risk of inflammatory bowel disease. Eur J Gastroenterol Hepatol, 11(5),543-546. Frank D. N., St Amand A. L., Feldman R. A. et al (2007). Molecular-phylogenetic characterization of microbial communities