This is an automatically translated article.
Article by Master, Doctor Nguyen Manh Ha - Radiotherapy Doctor - Radiation Therapy Center - Vinmec Times City International General Hospital.Ha Ngoc Son*, Tran Ba Bach1, Nguyen Dinh Long1, Chu Van Dung2, Pham Tuan Anh2, Nguyen Van Han2, Nguyen Van Nam2, Nguyen Trung Hieu2, Doan Trung Hiep3, Nguyen Manh Ha3
Summary
Objective: Evaluation daily setting error using 3D-CBCT image data to determine Setupmargin in 4D-DIBH radiotherapy (end-inspiratory hold) for left breast cancer.
Subjects and methods: A total of 13 patients with left breast cancer indicated for radiotherapy through the Tumorboard from July 2018 to August 2020 at Vinmec Times City International General Hospital . The patients were divided into two groups: Group 1- Had left breast-conserving surgery, Group 2- Total left mastectomy. The patient underwent a simulated CT scan on an Optima 580, using an RPM breathing management system and a Breast board immobilizer kit for breast cancer radiotherapy. Daily 3D-CBCT verification while the patient is holding their breath at the end of maximal inspiration, using the OBI system on the Clinac iX accelerator. A total of 181 3D-CBCT image sequences for group 1 subjects and 149 3D-CBCT image sequences for group 2 subjects were compared with simulated CT images.
Results: In 181 sets of CBCT images for subjects in group 1, the mean and SD of patient setup error were: 2.64 ± 3.87 mm (maximum 14 mm), 2.1 ± 3.15 mm (max. 12 mm), 2.86 ± 3.73 mm (max. 12 mm) in AP, SI, LR directions respectively. In total 149 sets of CBCT images for subjects in group 2, the mean and SD of patient setup error were: 1.88 ± 2.89 mm (maximum 15 mm), 1.99 ± 2.96 mm (maximum 14 mm) ), 3.74 ± 4.39 mm (up to 16 mm) in the AP, SI, LR directions respectively.
Conclusion: Setup margin for groups 1 and 2 is 6.43mm, 3.67mm, 7.26mm respectively in AP, SI, LR directions. SM for group 2: 4.91mm, 5.09mm, 9.45mm objects in AP, SI, LR directions respectively. This is an important basis for doctors and engineers to calculate and give an appropriate PTV margin for radiation therapy for left breast cancer using 4D-DIBH technique.
*, 2 Radiotherapy Technician, 1 Radiotherapy Engineer, 3MSc.BS. Head of Radiation Therapy Department - Department of Radiation Therapy, Vinmec Times City International General Hospital.
Contact: v.sonhn1@vinmec.com. Phone: (+84) 972,426,882.
Abstract
Objectives : To evaluate the setup error and daily movement used 3D-CBCT imaging data to determine Setup margin in 4D-DIBH radiotherapy ( Deep Inspiration Breath Hold) for left breast cancer.
Materials and methods : A total of 13 patients with left breast cancer are receiving radiotherapy through the Tumorboard from July 2018 to August 2020 at Vinmec Times City International Hospital. The patients were divided into two groups: Group 1- had surgery to preserve the left breast, Group 2 had surgery to remove the left breast completely. Patient was simulated CT scan on Optima 580, using the RPM breathing management system and the Breast board immobilizer kit for breast cancer radiation therapy. Daily 3D-CBCT verification while the last breath-holding patient inhales maximum, using the OBI system on the Clinac iX accelerator. A total of 181 3D-CBCT image sequences for group 1 objects and 149 3D-CBCT image sequences for group 2 subjects were analyzed and compared with simulated CT images.
Results : Of the 181 sets of CBCT images for group 1 subjects, the mean and SD of the patient setup error were: 2.64 ± 3.87 mm (up to 14 mm), 2.1 ± 3.15 mm (up to 12). mm), 2.86 ± 3.73 mm (maximum 12 mm) in the respective AP, SI, LR directions. A total of 149 sets of CBCT images for group 2 subjects, the mean and SD of the patient setup error were: 1.88 ± 2.89 mm (maximum 15 mm), 1.99 ± 2.96 mm (up to 14 mm) 3.74 ± 4.39 mm (maximum) 16 mm) in the AP, SI, LR directions respectively
Conclusion : The setup margin for groups 1 and 2 is 6.43mm, 3.67mm, and 7.26mm respectively in the AP, SI, LR directions respectively. SM for group 2 objects: 4.91mm, 5.09mm, 9.45mm in the directions AP, SI, LR respectively. This is an important basis for doctors and engineers to calculate and propose the appropriate PTVmargin level for radiation therapy for left breast cancer using 4D-DIBH
1. Make a problem
Breast cancer is the second most common cancer in terms of incidence and fifth in mortality in the world (Global Cancer 2018), for women breast cancer is the leading type in terms of risk.
Due to the anatomical location of the heart, patients receiving radiation therapy for left breast cancer have a higher risk of heart disease due to radiation-contaminated heart tissues. Long-term side effects and improving the quality of life for patients are also concerns of radiation therapists. Modern radiation therapy techniques: VMAT, IMRT were born with the aim of reducing radiation exposure to the heart, however, it is not possible to completely avoid all cardiac tissues and structures when treating left breast cancer
Radiation therapy 4D-DIBH (Deep Inspiration Breath Hold) holding your breath at the end of maximal inspiration is a recognized method for achieving this. The technique (DIBH) increases lung volume, increases the distance between the heart and the chest wall in irradiated fields, reduces the effective dose to the heart, and reduces the volume of the irradiated lung. Multiple studies have shown a dose-measured benefit of DIBH treatment in reducing cardiac dose compared with standard free-breathing therapy. Thus, DIBH has been widely accepted as one of the left breast radiotherapy techniques to minimize cardiac dose
Although the benefits of DIBH have been well recognized, issues such as the ability to reproduce the degree of silence Breathing, correct posture, and patient cooperation are limiting factors. In order to ensure the accuracy of daily irradiation, we conduct research to evaluate the ability to re-establish the level of breath holding, treatment position, thereby determining a separate Setup margin for breast cancer treatment. Left using 4D-DIBH technique at Vinmec times city radiotherapy center.
2. Objects and methods
Subject
A total of 13 patients with left breast cancer with indications for radiation therapy through the Tumorboard from July 2018 to August 2020 at Vinmec Times City International General Hospital. The patients were divided into 2 groups: Group 1 - Left breast-conserving surgery, Group 2 - Left mastectomy.

Bảng 1. Thông tin bệnh nhân
CT scan simulating breathing (BH: Breath Hold): The patient is placed in the supine position with the head above using the Breast board immobilizer system, the left hand is perpendicular to the body, the table slope is 50, support at arm and wrist. To limit mobility in the direction of the head and foot, the patient's buttocks are padded close to the buttocks, the legs are rested on the knee fix. An RPM (Real-Time position management) breathing synchronization system including camera and marker block (Varian Medical Systems, Palo Alto, CA) was used for the BH technique. The Maker block is placed 2 fingers below the sternum and is marked right after the end of the simulation. Ensure the marker placement is fixed during all treatments. Before the simulation, the patients were trained in breathing management procedures, chest breathing pattern, stable breathing amplitude, patients holding their breath at the end of the maximal inhalation, holding breath for 15-20 seconds, repeating the cycle. at least 5 times. Simulated CT scan on an Optima 580 (GE Medical System, Milwaukee, Wisconsin USA). A series of simulated CT scans were performed with the patient holding their breath at the end of maximal inspiration.

Đặt tư thế và cố định bệnh nhân

Tín hiệu biên độ thở của bệnh nhân trong chụp CT mô phỏng nhịn thở
Daily radiation therapy: Before daily irradiation according to the approved plan, patients were photographed to verify 2D-kV matching according to bone landmarks to assess breathing amplitude, posture and treatment position. Table translation is not carried out due to limitations of the treatment machine system. 3D-CBCT matching according to soft tissue, focusing on PTV to ensure accuracy in dose delivery. A total of 330 CBCT sequences were obtained for both groups, which were used to analyze postural setting errors during daily radiotherapy.

Xác minh hình ảnh 2D-kV theo hướng LR và hướng AP
. Xác minh hình ảnh 3D-CBCT matching theo mô mềm

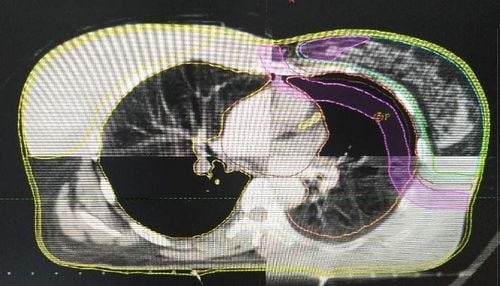
So sánh sai số giữa hình ảnh mô phỏng và hình ảnh CBCT theo dải màu, màu càng đậm thể hiện sai số càng lớn.
Methods
Retrospective study method.
Based on the comparison of 3D-CBCT images with the original soft tissue simulation CT images (usually using PTV), the daily change of treatment position was recorded.
Installation error calculated by van Herrk formula: SMvanHerk = 2.5 Σsetup +0.7 σsetup where: setting error (SMvanHerk: setup margin) systematic error (Σ: systematic error) is determined by standard deviation of the mean setting errors for each patient, the random error (σ: random error) is determined by the average of the standard deviations for each patient.
3. Results and discussion
Setting error
In 181 sets of CBCT images for subjects in group 1, the mean and SD of the patient setting error were: 2.64 ± 3.87 mm (maximum 14 mm), 2.1 ± 2 3.15 mm (max. 12 mm), 2.86 ± 3.73 mm (max. 12 mm) in AP, SI, LR directions respectively. In total 149 sets of CBCT images for subjects in group 2, the mean and SD of patient setup error were: 1.88 ± 2.89 mm (maximum 15 mm), 1.99 ± 2.96 mm (maximum 14 mm) ), 3.74 ± 4.39 mm (up to 16 mm) in the AP, SI, LR directions respectively. Setup margin according to van Herk's formula for patients in group 1: 6.43mm, 3.67mm, 7.26mm in AP, SI, LR directions respectively. SM for group 2: 4.91mm, 5.09mm, 9.45mm objects in AP, SI, LR directions respectively. Summarize errors by group in tables 2 and 3.
Table 2. Errors set in 3 directions -Group of patients 1.
| Hướng | Vrt (AP) mm | Lng (SI) mm | Lat (LR) mm |
|---|---|---|---|
| Sai số trung bình | 2.64 | 2.10 | 2.86 |
| Sai số lớn nhất | 14 | 12 | 12 |
| Sai số hệ thống, ∑SM | 1.62 | 0.68 | 2.08 |
| Sai số ngẫu nhiên, σSM | 3.41 | 2.82 | 2.92 |
| Setup Margin (van Herk) | 6.43 | 3.67 | 7.26 |

Biểu đồ thể hiện xu hướng sai số cài đặt xảy ra theo 3 hướng-Nhóm BN 1
Table 3. Setting error in 3 directions -Patient group 2.
| Hướng | Vrt (AP) mm | Lng (SI) mm | Lat (LR) mm |
|---|---|---|---|
| Sai số trung bình | 1.88 | 1.99 | 3.74 |
| Sai số lớn nhất | 15 | 14 | 16 |
| Sai sô hệ thống, ∑SM | 1.27 | 1.34 | 2.85 |
| Sai số ngẫu nhiên, σSM | 2.48 | 2.50 | 3.31 |
| Setup Margin (van Herk) | 4.91 | 5.09 | 9.45 |

Biểu đồ thể hiện xu hướng sai số cài đặt xảy ra theo 3 hướng-Nhóm BN 2
4. Discussion
Some studies demonstrate that using 2D image data: 2D kV, 2D-MV to verify the location of treatment matching according to bone landmarks for radiation therapy for left breast cancer is not enough because the whole breast has can move independently of the thoracic wall. Therefore, it is necessary to use 3D-CBCT to verify daily irradiation site for left breast cancer radiotherapy using 4D-DIBH technique.
Holding the breath helps to increase the thoracic volume, increasing the distance between the heart and the chest wall, but it can also be the cause of the patient's position shift.
In our study for both groups of subjects, the error in the anterior and posterior direction was quite stable, showing that the re-establishment of breathing amplitude, breathing management was done very well. In addition, the errors mainly occurred in the LR direction (Left and Right) in both groups, which very accurately reflected the limitations of the current system of fixed posture devices (Breast board), which is the ability to control poor bilateral mobility. The fixed use of Vaclok will better assist in restricting movement in the horizontal direction. In addition, the Surface guide system will be the best option in controlling the movement before and during the treatment to ensure the accuracy and effectiveness of the treatment process.
4D-DIBH radiotherapy technique has shown many outstanding advantages compared to conventional radiotherapy techniques for left breast cancer, however, to widely apply the technique requires synchronous basic Material equipment, operating experience besides the problem of treatment time for each patient will be longer than standard radiation therapy methods (average treatment time 25-30 minutes) is also a problem. quite a big barrier that radiotherapy centers need to consider.
5. Conclusion
Daily use of CBCT in conditioning to minimize setup errors for left breast cancer radiotherapy using 4D-DIBH radiotherapy technique is essential. Setup margin for groups 1 and 2 is 6.43mm, 3.67mm, 7.26mm respectively in AP, SI, LR directions. SM for group 2: 4.91mm, 5.09mm, 9.45mm objects in AP, SI, LR directions respectively. This is an important basis for doctors and engineers to calculate and give an appropriate PTV margin for radiation therapy for left breast cancer using 4D-DIBH technique.
REFERENCES:
T.J. Whelan, J. Julian, J. Wright, et al. Does locoregional radiation therapy improve survival in breast cancer? A meta-analysis Clin 0ncol, 18 (2000), pp. 1220-1229 M. Clarke, R. Collins, S. Darby, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomized trials Lancet, 366 (2005), pp. 2087-2106 S.C. Darby, P. McGale, C. Correa, C. Taylor, R. Arriagada, M. Clarke, D. Cutter, C. Davies, M. Ewertz, J. Godwin, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomized trials Lancet, 378 (2011), pp. 1707-1716 P. McGale, C. Taylor, C. Correa, D. Cutter, F. Duane, M. Ewertz, R. Gray, G. Mannu, R. Peto, T. Whelan, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: Meta-analysis of individual patient data for 8135 women in 22 randomized trials Lancet, 383 (2014), pp. 2127-2135 M.J. Hooning, A. Botma, B.M. Aleman, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer J Natl Cancer Inst, 99 (2007), pp. 365-375 B. Offersen, I. Hojris, M. Overgaard Radiation-induced heart morbidity after adjuvant radiotherapy of early breast cancer – Is it still an issue? Radiother Oncol, 100 (2011), pp. 157-159
S.C. Darby, P. McGale, C. W. Taylor, et al. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: Prospective cohort study of about 300,000 women in US SEER cancer registries Lancet Oncol, 6 (2005), pp. 557-565 Sardaro, M.F. Petruzzelli, M.P. D'Errico, L. Grimaldi, G. Pili, M. Portaluri Radiation-induced cardiac damage in early left breast cancer patients: risk factors, biological mechanisms, radiobiology, and dosimetric constraints Radiother Oncol, 103 (2012), pp. 133-142 A.C. Darby, M. Ewertz, P. McGale, A.M. Bennet, U. Blom-oldman, D. Bronnum, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer N Eng J Med, 368 (2013), pp. 987-998 Y.H. Lee, J.S. Chang, I.J. Lee, et al. The deep inspiration breath hold technique using ABC reduces cardiac doses in patients undergoing left-sided breast irradiation Radiat Oncol J, 31 (2013), pp. 239-246 T. Swanson, I.S. Grills, H. Ye, et al. Six-year experience routine using moderate deep inspiration breath-hold for the reduction of cardiac dose in left-sided breast irradiation for patients with early-stage or locally advanced breast cancer Am J Clin Oncol, 36 (2013), pp. 24-30 A.J. Hayden, M. Rains, K. Tiver Deep inspiration breath hold technique to reduce heart dose from radiotherapy for left-sided breast cancer J Med Imaging Radiat Oncol, 56 (2012), pp. 464-472 M.H. Hjelstuen, I. Mjaaland, J. Vikstrom, K.I. Dybvik Radiation during deep inspiration allows loco-regional treatment of left breast and axillary-, supraclavicular- and internal mammary lymph nodes without compromising target coverage or dose restrictions to organs at risk Acta Oncol, 51 (2012), pp. 333-344 W. Wang, T.G. Purdie, M. Rahman, A. Marshall, F.F. Liu, A. Fyles Rapid automated treatment planning process to select breast cancer patients for active breathing control to achieve cardiac dose reduction Int J Radiat Oncol Biol Phys, 82 (2012), pp. 386-393 J. Vikstrom, M.H. Hjelstuen, I. Mjaaland, K.I. Dybvik Cardiac and pulmonary dose reduction for tangentially irradiated breast cancer, utilizing deep inspiration breath-hold with audio-visual guidance, without compromising target coverage Acta Oncol, 50 (2011), pp. 42-50