The article is professionally consulted by Master, Doctor Tong Van Hoan - Emergency Medicine Doctor - Emergency Department - Vinmec Danang International Hospital.
Emergency pleurodesis is a procedure where a sterile tube is inserted into the pleural space, connected to a closed system, to aspirate air or fluid present in the pleural space. Purpose: Restore negative pressure in the pleural cavity, pulmonary expansion Prevent the risk of hemodynamic disturbances due to pneumothorax, pressure-type hemothorax The purpose of treatment and monitoring in purulent effusion hemothorax
1. What is emergency pleurodesis?
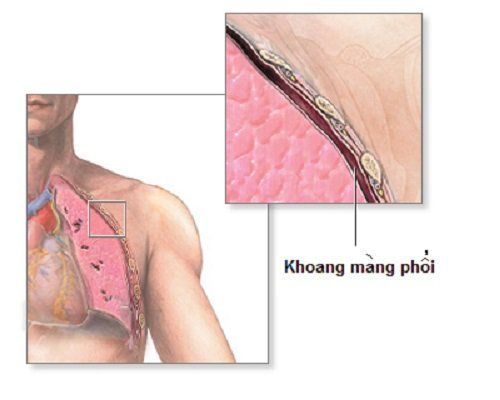
The pleura is a virtual cavity formed by the parietal and visceral pleura. Under normal conditions, pleural pressure is in the range of -2 to -4 mmHg, varying with inspiration and expiration. Minimal pleural effusion is a procedure performed to free the pleural space from fluid or air pressure by inserting a flexible, hollow tube, draining air or fluid through the chest wall, and bringing the pleural cavity into place. to the initial state is a virtual cavity with negative pressure. The procedure for performing emergency pleurectomy must ensure 4 principles: hermetic, aseptic, one-way and continuous suction with controlled pressure in the range -20cm H2O to -30cm H2O.
2. Indications/contraindications for emergency pleural effusion
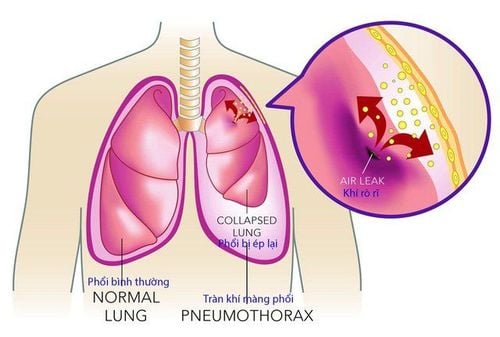
2.1 Indications for emergency thoracentesis Pneumothorax with one of the following conditions
Tình trạng tràn khí màng phổi
Pneumothorax in patients with artificial ventilation; Pneumothorax with a large amount; Pneumothorax in patients with unstable clinical symptoms; Pneumothorax due to trauma; Tension pneumothorax; Persistent or recurrent pneumothorax; Pneumothorax by doctor; Pneumothorax due to failure of aspiration measures, placement of airways; Hemothorax due to trauma or complications after the procedure; Esophageal pleural fistula; Pleural effusion has a rapid recurrence; Pleural effusion due to cancer; Empyema should be drained and the pleural cavity washed; Causing pleural adhesions through the drain; Nourish the pleura; Pleural drainage after thoracic surgery.
Bệnh nhân bị tràn dịch màng phổi
2.2 Contraindications There are no absolute contraindications for pleural effusion, except in cases where the patient has a medical condition that causes the lung to completely adhere to the chest wall. Relative contraindications in cases where the patient is at risk of bleeding due to clotting disorders and taking anticoagulants. In these cases, the procedure can be performed when there are enough transfusions of clotting factors and platelets. to ensure that bleeding risk is low or higher (platelets > 60 G/L and APTT disease/control < 1.5).
3. Perform emergency pleurodesis
Emergency thoracentesis steps need to be strictly followed to ensure the best treatment results. 3.1 Prepare the Performer: Technically proficient respiratory therapist and nurse. Facilities: pleural drainage tube size 28 - 31G, pleural opening kit, sterile cuff, sterile gloves, 1.5% iodide alcohol, 70° white alcohol, anesthetic, drugs and emergency equipment according to indicated, 20ml syringe, gauze, scalpel, needle, suture needle, one-way air or closed-loop suction aspirator. Patient: Need an explanation of the purpose of the procedure; signed a commitment to consent to the procedure; psychological encouragement; give snacks; have the patient go to the toilet; Xylocaine reaction test; intramuscular injection of Atropin 1/4mg about 15 - 30 minutes before the procedure; inject pain medication about 15 minutes before the procedure. The patient needs to lie in a standard position: Lie on your back, straight, with your head high, and raise your hand above the affected lung. Depending on the case, the patient can lie with the head elevated, prone or sitting. Medical record: Full results of subclinical investigations such as chest X-ray film, computed tomography film, basic coagulation, blood count test results, urea, creatinine, ALT, ADT, electrocardiogram solve map.
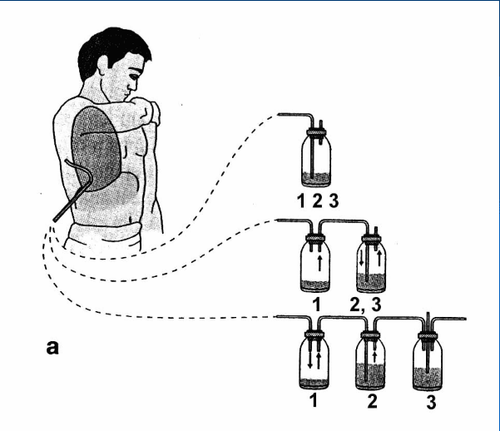
Hệ thống dẫn lưu màng phổi một chiều
3.2 Perform the technique Wash hands, wear gloves Disinfect the drainage site with Betadin, alcohol Sterile cloths Anesthetize layers: skin, pleural muscle, pleural cavity, the principle of anesthesia is to start from the horizontal. rib just below the intercostal space intend to drain gradually and go deep into that intercostal space Using a scalpel to make a skin incision at the transverse position of the rib 5 middle axillary, the length of the incision is 1.5 to 2cm, making an incision through the skin to the muscle layer. Using a curved Pinch with a blunt end (Kelly) to dissect each layer of muscle in the direction from the level of the ribs to the intercostal space and deep into the pleural space When reaching the pleural space, there will be a feeling of "Hung" in the hand and there is air or fluid. out Use the finger of 1 hand to insert into the pleural cavity to probe and check the drainage has entered the pleural cavity and at the same time can dissect a part of the pleural space if there is adhesion at the drainage site After making sure pleural cavity, conduct catheterization of Sonde tube: Use a curved Pinke to clamp the tip of the drain tube along the upper opening line, when entering the pleural cavity, there will be fluid or gas through the duct. If air is vented, point the tip of the tube upwards. If the drain is to be drained, let the tip of the tube point down. Fix the drain. Connect the drain to the continuous suction system. Check the position of the drain. Take a chest x-ray to check the drain.
3.3 Monitoring Monitoring of the condition: During the procedure: Measure pulse, blood pressure and breathing rate, monitor facial expressions, see if the patient has chest pain, has difficulty breathing. After the procedure: Check pulse, blood pressure, respiratory rate and chest X-ray to evaluate the results of the procedure. Drain monitoring: After connecting the drain to the suction system, drain the fluid and calculate the hourly output. In the case of drainage without translation, it is necessary to check whether the drainage is clear. If the fluid column in the drainage tube fluctuates with the patient's breathing, the cyst is still clear and the fluid has been aspirated. Evaluation of drainage in terms of color, quantity, nature,...; Change and wash the drainage vessel every 24 hours or when the fluid is full; Physical examination, chest x-ray to check if the lungs are enlarged after drainage. Withdrawal of drainage: In the case of pleural drainage: Based on chest X-ray images and clinical examination results, remove the drain tube when the amount of drainage is less than 50ml/24h and the color of the fluid is clear. In the case of pneumothorax: Clamp and withdraw the drainage according to standard technical procedures. Drainage technique: When withdrawing, the drain must be continuously aspirated until the tube is completely withdrawn from the pleural space to remove the remaining air and fluid in the tube and in the pleural space. Ligation waits immediately after extubation, disinfect with betadin and carefully bandage. Make an appointment for the patient to re-examine after 1 week to remove the waiting thread. Monitor complications including: bleeding, organ injury, infection...
Hình ảnh X-quang phổi
3.4 Complications and management Chest pain: Management by using analgesics. Bleeding due to puncture of the intercostal nerve bundle: Surgical intervention is possible if necessary. Wrongly poked into adjacent organs such as lung, spleen, liver, stomach,...: Preventive measure is to master the anatomical position, determine the exact location of pleural opening based on X-ray film. , thoracic computed tomography, ultrasound of the pleural cavity. Treatment according to the doctor's plan. Fear-induced syncope: Prevent by explaining to the patient well before the procedure for good coordination and giving a light snack before the procedure. Acute pulmonary edema: Usually occurs when aspiration is high, the fluid drains too quickly and a lot, and is treated according to the standard protocol of the doctor. Infection: Due to non-compliance with the principle of sterility in the procedure, the treatment is strictly according to the standard protocol of the doctor. Other complications: Obstruction of drainage ducts, subcutaneous emphysema, etc., properly handled according to the doctor's protocol. Note: Do not aspirate fluid, gas with high pressure and the amount of more than 1 liter/1 time. When being assigned to perform an emergency pleural technique, the patient needs to cooperate well with the doctor to ensure the procedure is successful and minimize the risk of unwanted complications. Vinmec International General Hospital currently has a modern emergency thoracotomy technique performed by a team of qualified and experienced medical doctors, with a complete and advanced medical equipment system will give the best treatment results.
Định kỳ kiểm tra sức khỏe giúp phát hiện và điều trị sớm bệnh lý
Master. Doctor Tong Van Hoan has 10 years of experience in the field of Emergency Resuscitation, is capable of performing difficult techniques in Emergency Resuscitation such as advanced mechanical ventilation, continuous and intermittent dialysis, plasma exchange. , difficult airway intervention, hemodynamic monitoring by PiCCO, advanced cardiopulmonary resuscitation (ACLS), emergency bedside ultrasound, echocardiography... For detailed advice on laparotomy technique For emergency lung at Vinmec, please go directly to Vinmec health system or register online HERE. MORE: Emergency pleural ultrasound Diseases that can be diagnosed early with a chest X-ray What is an X-ray: All you need to know
The drug Bedexlor has 2 main ingredients, Betamethasone and Dexchlorpheniramine maleate, which is prepared in the form of tablets. Bedexlor is used in the treatment of allergies, severe bronchial asthma, allergic rhinitis, ....
Pleural ultrasound is an imaging technique aimed at diagnosing chest wall diseases, pleural effusion, pleural tumors, pneumothorax... Pleural ultrasound is always convenient and quick to perform.
Bleomycin sulfate is an antibiotic against cancer, including Hodgkin lymphoma, non-Hodgkin lymphoma, testicular cancer, ovarian cancer and cervical cancer. Similar to other cancer drugs, Bleomycin sulfate is available by injection into a vein, into a muscle, or under the skin.
Nowadays, X-ray plays a very important role in diagnosing and treating diseases. This method helps doctors observe the inside of the patient's body without having to operate. The following article will help us have the most complete understanding of X-ray.
Hepatobiliary abscess is a disease with a relatively small incidence, but the danger to the health and life of the patient is inevitable and is of great concern to many people. Because there are many ways to attack the liver, bacteria are thought to be the leading cause of this disease.
Thoracentesis is intended to remove fluid, blood, pus, and air in the pleural cavity that causes acute respiratory failure. This is a difficult procedure, requiring the performer to have professional skills and the facility to have modern technical facilities. In addition, to ensure that the steps of performing emergency thoracentesis limit complications, the patient must follow the doctor's instructions.