This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International HospitalStomach cancer that is not caused by H. pylori infection is quite low but makes it difficult to diagnose. Depending on your symptoms, your doctor will perform an exam and use appropriate imaging methods.
Abbreviation:
H. pylori-associated gastric cancer (HpPGC)
Stomach cancer not caused by H. pylori infection ( Stomach cancer not caused by H. pylori infection )
1. Frequency of gastric cancer not due to H. pylori infection
The frequency of gastric cancer not due to H. pylori infection is low, but this number is expected to increase and the frequency of gastric cancer not due to H. pylori infection may increase accordingly. Currently, gastric cancer not due to H. pylori infection is still rarely reported and the frequency varies considerably from 0.66% to 14% of gastric cancer cases. The difference in this range may be due to differences in the definition of H. pylori-free status in previous reports.2. H. pylori detection methods
Methods for the detection of H. pylori have high sensitivity and specificity and are generally divided into invasive (endoscopic-based) and non-invasive methods. Invasive diagnostic tests include endoscopic imaging, histology, culture, and molecular methods. Non-invasive diagnostic tests include H.Pylori C13 breath test, stool antigen test, serological and molecular testing. The accuracy of diagnosing H. pylori infection varies depending on the test. The sensitivity and specificity of UBT, serum anti-HP-IgG antibodies were 95% and 95%, 91%-100% and 50%-91% and 85%-95% and 95%-100%, respectively. , however, some tests may produce false negatives due to Proton Pomp Inhibitors (PPIs) or patient factors, including past antibiotic use. To confirm H. pylori uninfected status, multiple tests are needed to demonstrate, even if the patient is currently negative for H. pylori . Because there is a possibility that the patient has had a past infection, evaluation of gastric atrophy is necessary to differentiate and determine if there has been an infection in the past.3. Diagnosis of gastric cancer due to H.pylori infection by magnifying endoscopy with narrow band imaging (ME-NBI)
Magnified endoscopy with narrow band imaging (ME-NBI) is a recently developed technique. This is a combination of magnified endoscopy and narrow band imaging. It is widely used in the detection of esophageal and gastric cancers based on the basic microscopic findings of the microvascular (MV) and microscopic surface (MS) structures of the superficial mucosa. The gastric mucosa is composed of glandular epithelium, which is different from normal glands. There are different classification systems to describe the correlation between the microscopic image and the actual image displayed using ME-NBI.4. MV (Microvascular) and MS (Microsurface) models and boundaries in early gastric cancer diagnosis
The MV (Microvascular) and MS (Microsurface) models were reported by Yao et al., in which three microvascular/microsurface patterns are described: regular, irregular and do not have. According to these MS/MV patterns, one can differentiate gastric low-grade dysplastic adenomas from early gastric cancer or determine the extent of lateral spread and depth of tumor invasion of gastric cancer. early thickening for laparoscopic resection. The diagnostic criteria for gastric cancer depend on the presence of an irregular MS/MV pattern with a demarcation line.It is worth mentioning that 97% of EGCs fit the above criteria. Kaise et al examined the significance of various MS and MV changes, such as disappearance of the MS pattern, variation in vessel size, and conformational heterogeneity. These criteria confirmed the diagnosis of cancer with sensitivity of 69.1% and specificity of 85.3%. To distinguish between adenocarcinoma and undifferentiated adenocarcinoma, Nakayoshi classified MV models of superficial gastric cancer into three groups: small reticular model, spiral model and unclassified model. Yokoyama et al found that the intraocular loop (Karaoke) pattern and the presence of fine meshwork or torsion vessels on the MV model may be related to the histologic subtype, but it is unclear whether these criteria can be widely applied.
Mô hình MV (Microvascular) và MS (Microsurface): Hình ảnh một tổn thương ung thư sớm ở dạ dày, với đường ranh giới (Dermacation line), bất thường vi bề mặt (Microsurface) và vi mạch máu (Microvascular)
5. Difficulty in diagnosing gastric cancer not caused by H.pylori . infection
The anomalous neoplastic changes in gastric cancer not due to H.pylori ME-NBI infection are due to the fact that tumor cells exist only in the proliferative region of the mucosa and the surface layer is covered by non-epithelial epithelium. cancer. This is why pathological findings do not show abnormalities in microvessels/microsurfaces. Immunologically, the tumor cells showed a gastric phenotype. It is known that ring cell carcinoma indicative of an intestinal phenotype invades from the proliferative region of the mucosa into the deep mucosa and individually invades the submucosa while maintaining the muscular mucosa and sometimes progression to gastric cancer. Ring cell carcinoma of the stomach, which progresses from the proliferative region to the superficial layer of the mucosa, has a lower malignant potential than the intestinal phenotype.
Ung thư biểu mô tuyến dạng tuyến cơ bản ở dạ dày không nhiễm H.pylori
6. It is possible to misdiagnose stomach cancer that is not caused by H. pylori infection with some other diseases
Previous reports of differentiated non-H. pylori gastric cancer mostly identified basal adenocarcinoma and gastric phenotype gastric cancer with low-grade muscular atrophy. . However, given the small number of reports, it is difficult to define consistent clinical features of gastric cancer not due to H. pylori infection.It is worth noting that, in addition to ring cell carcinoma alone and basal adenocarcinoma, commonly seen in previous reports, the authors' study also included adenocarcinoma rheumatic gastric phenotype, focal adenocarcinoma and intestinal adenocarcinoma. The occurrence of basal adenocarcinoma types has been reported in addition to the undifferentiated type in previous reports of gastric cancer not due to H. pylori infection. This tumor has a gastric phenotype and low-grade adenocarcinoma occurs in the basal gland above the midmucosal layer or just above the mucosal muscle layer. The tumor is covered with noncancerous epithelium, therefore, it exhibits a submucosal (SMT-like) tumor-like morphology and sometimes infiltrates the submucosa.

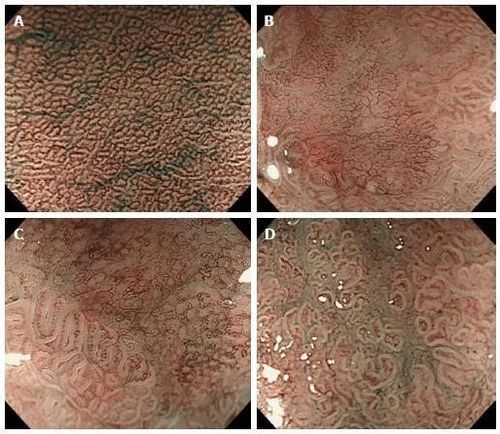
Ung thư biểu mô tuyến ruột

Ung thư biểu mô tuyến dạng phế nang. Hình A: Cấu trúc lông nhung bao gồm các tế bào trụ loạn sản với tế bào chất rõ ràng. Hình E: Một dạng niêm mạc mịn như nhú hoặc lông nhung với các mạch không đều cấu trúc bên trong ở tất cả các tổn thương, một tổn thương cho thấy hình dạng giống quả mâm xôi, nội soi phóng đại với hình ảnh dải hẹp; F: Một tổn thương có biểu hiện giống quả mâm xôi.
However, in this type of gastric cancer that is not caused by H. pylori infection, there are many cases that cannot be characterized by the usual classification of gastric cancer by NBI. For example, in basal adenocarcinoma, the dermacation line is not clear because the tumor is covered with non-neoplastic epithelium, so the pattern of surface microstructural abnormalities (is Frequent and typical NBI findings of well-differentiated adenocarcinoma) could not be determined. In addition, pure ring cell carcinoma does not exhibit the typical helical pattern, a microsurface variation of gastric cancer. These cases are classified according to the NBI classification system. Therefore, gastric cancer not caused by H. pylori infection may not fit the conventional NBI classification system.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
Reference1. Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, Taniyama K, Sasaki N, Schlemper RJ. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med . 2001;345:784-789. [PubMed] [DOI]
2. Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 7-14 June 1994. IARC Monogr Eval Carcinog Risks Hum 1994; 61: 1-241. [PubMed]
3. Chiko Sato, Kingo Hirasawa et al., Clinicopathological features of early gastric cancers arising patients in Helicobacter pylori uninfected patients, World J Gastroenterol. May 28, 2020; 26(20): 2618-2631