This is an automatically translated article.
Closed abdominal trauma can cause serious damage to the diaphragm such as a ruptured diaphragm. Diaphragmatic suture is an effective emergency treatment for this condition.
1. When is the diaphragm injured?
Closed abdominal trauma is often caused by traffic accidents, work accidents, conflicts, daily life or closed pressure pumps. Patients with blunt abdominal trauma often have symptoms of abdominal pain, abdominal distention, blood loss, infection, skin abrasions or bruising of the abdominal wall,...
Closed abdominal trauma can cause damage to many people. internal organs such as liver, pancreas, spleen, kidney,... and even the diaphragm.
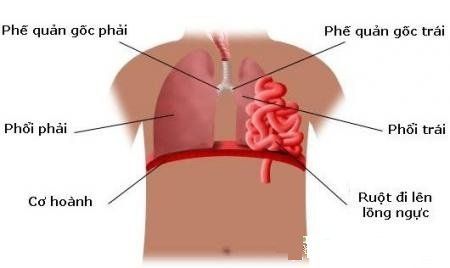
The diaphragm is a flat, wide, ring-shaped muscle, forming a tendon-muscle wall, separating the rib cage and the abdomen. The diaphragm plays a very important role in the physiology of the respiratory system. When the diaphragm contracts, the dome of the diaphragm lowers, helping the ribcage to expand, the pressure in the chest decreases to inhale air and vice versa. When the diaphragm is damaged, it will greatly affect the flow of air in and out of the lungs, leading to respiratory failure.
Closed abdominal trauma can cause perforation, rupture, and hernia of the diaphragm. When abdominal trauma, the diaphragm is damaged by the following mechanisms:
Strong and sudden increase in intra-abdominal pressure, central rupture of the diaphragm; Perforated broken ribs or puncture wounds to the diaphragm; Abdominal viscera can herniate into the thorax and cause strangulation.
2. Types of diaphragm damage due to blunt abdominal trauma
2.1 Perforation of diaphragm due to wound
Wounds to the thorax from the IV intercostal space down can cause perforation of the diaphragm. If the wound hole is more than 1.5cm in diameter, the viscera in the abdomen can pass through the wound hole to the pleural space.
Patients with diaphragmatic perforation may have the following symptoms:
Nasosternal pain; See digestive juices, bile, intestinal loops, omentum, ... in the wound hole in the chest wall; Acute asphyxia, cardiac arrhythmia, pale mucous membranes, ... when the viscera in the abdomen pass through the hole in the diaphragm into the thorax and cause compression of the internal organs in the chest cavity; Symptoms of intestinal obstruction caused by bowel loops being blocked at the diaphragmatic perforation. Patients with diaphragmatic perforation are usually indicated for exploratory laparotomy. When performing, it is necessary to endotracheal anesthesia to avoid complications of lung compression because when opening the abdomen, air enters the pleura through the hole in the diaphragm.

Thủng cơ hoành gây loạn nhịp tim
2.2 Diaphragm rupture
Diaphragm rupture is common due to strong trauma causing sudden increase in intra-abdominal pressure, causing the diaphragmatic arch to stretch and rupture. Usually the left diaphragm is more prone to rupture because the right diaphragm is covered by the liver. Through the diaphragmatic tear, the viscera in the abdomen can enter the ribcage, causing a diaphragmatic hernia due to trauma.
Symptoms of diaphragmatic tear often include:
Shortness of breath, pain in the damaged chest area, purple mucous membranes, arrhythmia, shock, ... because the abdominal organs pass through the hole in the diaphragm into the chest. cause mediastinal compression; Symptoms of intestinal obstruction due to bowel loop obstruction at the diaphragmatic tear. All cases of diaphragmatic tear require surgery to suture the tear. If the tear is extensive, it may need to be patched with artificial materials.
2.3 Diaphragm hernia
This is a condition in which the abdominal organs move up into the thorax through the diaphragmatic hernia. Diaphragmatic hernias usually occur after some time of trauma. Herniated viscera are usually the stomach, colon, small intestine, omentum, spleen, liver,... Herniated viscera are usually attached to the hernia hole and organs located in the chest such as pleura, pericardium, etc. ...
Symptoms of diaphragmatic hernia:
Epigastric pain or pain on one side of the chest and spread to the shoulder blade on the same side; There is a sound of bowel movements on the chest; There are symptoms of intestinal obstruction due to intestinal loop strangulation at the hernia opening; Shortness of breath increases when lying down. Sometimes patients have severe shortness of breath, cyanosis of the mucous membranes due to the large hernia causing compression of the mediastinum, heart and lungs. Diaphragmatic hernia should be indicated for early surgery. The patient was given endotracheal anesthesia to bring the herniated organs back into the abdomen, then sutured the hernia hole with non-digestible sutures. In case of large hernia hole, surgery to reconstruct the diaphragm is required.
3. Diaphragm suture surgery in closed abdominal trauma
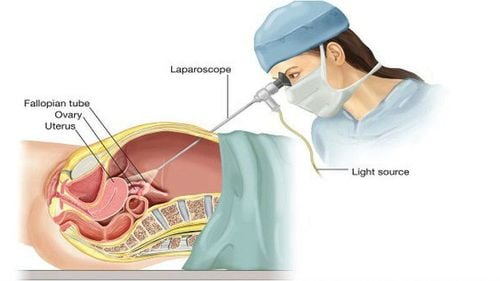
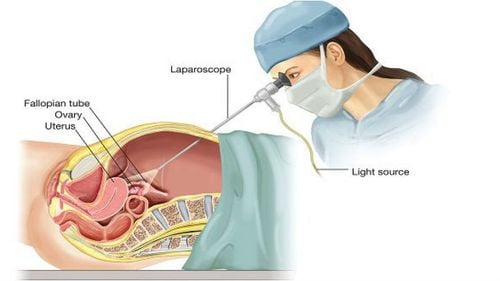
Diaphragm sutures can be performed via open surgery or thoracotomy/laparoscopic surgery. Laparoscopic surgery method has the advantages of reducing costs, shortening hospital stay, and returning the patient's labor soon.
3.1 Indications/contraindications
Indication
Person who is diagnosed with diaphragmatic rupture with sufficient clinical symptoms and X-rayed; The patient is eligible for laparoscopic surgery; Emergencies: The patient is carefully evaluated during laparoscopic surgery. Contraindications
Relative contraindications for people with visceral damage in the peritoneal cavity; Diaphragm rupture accompanied by hemodynamic disturbances; The patient's health is too weak to tolerate surgery; The patient is old and weak and has many co-morbidities; Contraindications to laparoscopic surgery: Localized or free ascites; surgical history of peritonitis, intestinal obstruction; local infection of the abdominal wall; abdominal wall hernia , umbilical hernia ; blood clotting disorders; Heart valve disease, coronary heart disease, chronic bronchial disease.

Người già có sức khỏe yếu chống chỉ định phẫu thuật
3.2 Preparation for surgery
Implementation personnel: Surgeons, anesthesiologists, resuscitation assistants; Technical facilities: synchronous equipment for laparoscopic surgery; Patient: The surgery is explained (purpose, procedure, risk of complications); basic tests, endoscopy, X-ray, abdominal ultrasound; Rehydration and electrolytes and use of prophylactic antibiotics before surgery; Medical records: Prepare according to regulations including detailed medical records, minutes of consultation, minutes of pre-anesthesia examination and written consent to surgery.
3.3 Performing surgery
Check records and patients, make sure the right person and the right disease; Patient position: supine, head high, legs low, legs apart, nasogastric tube placed; Anesthesia: Conduct endotracheal anesthesia; Place trocar: Trocar 10mm (for camera) placed through the umbilicus; 5mm trocar (for liver lifter and round ligament) placed on the right side of the sternum; trocar 5mm above the right breast line and 5cm below the costal margin; 5mm trocar placed across the navel on the left white line; Inflate the abdomen: 12 - 14 mmHg; Examination of the abdomen: Check and evaluate damage to the diaphragm and visceral organs in the peritoneal cavity; Diaphragm suture: Expose the ruptured diaphragm and bring the herniated viscera back into the abdominal cavity. Then, filter the broken edge of the diaphragm, suture the diaphragm with non-absorbable sutures with a separate stitch. Note, before suturing the diaphragm, it is necessary to place a pleural drainage. In case the rupture of the diaphragm is large, the suture is tight and the risk of recurrent diaphragmatic rupture is high, an artificial graft can be placed; Check, aspirate fluid, blood in the peritoneal cavity and close the trocar holes.
3.4 Follow-up after surgery
Give the patient antibiotics for 5-7 days; Feed the patient early from the 2nd day after surgery if there is no gastrointestinal intervention; From day 2, check chest X-ray for good lung expansion, then withdraw chest drainage; Pay attention to replenish water and electrolytes for the patient.

Sau phẫu thuật, bệnh nhân cần được chụp X-quang
3.5 Handling of accidents
Complications in surgery:
Bleeding: Treat by clamping the hemostatic clip; Gastrointestinal perforation: The treatment is to suture immediately during surgery; Complications after surgery:
Bleeding: Perform surgery to stop bleeding; Missing perforation of the gastrointestinal tract causing peritonitis: It is recommended to re-operate with drainage or suture the perforation depending on the patient's abdominal condition; Abdominal residual abscess: Perform ultrasound or computed tomography of the abdomen to identify an abscess. Then, depending on the size of the abscess, it is possible to treat with antibiotics or drain the abscess under the guidance of ultrasound. Injury to the diaphragm after blunt abdominal trauma is very dangerous, can lead to many unpredictable complications. Therefore, it is necessary to be alert to the risk of accidents causing closed abdominal trauma, and at the same time to quickly take the victim to the emergency room for timely intervention.
Any questions that need to be answered by a specialist doctor as well as customers wishing to be examined and treated at Vinmec International General Hospital, you can contact Vinmec Health System nationwide or register online HERE.