This is an automatically translated article.
Posted by Doctor Mai Vien Phuong - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.In daily diagnosis, we sometimes encounter endoscopic diagnoses of diaphragmatic hernia, in some severe cases requiring surgery. So where is the diaphragm? What is the diaphragm? Constructed how? This article will tell us the above information.
1. Diaphragm and diaphragmatic hernia
The diaphragm is a muscle that separates the abdominal cavity from the thoracic cavity. In this muscle, there are holes, slits, and recesses for the structures between the chest and abdomen to communicate with each other.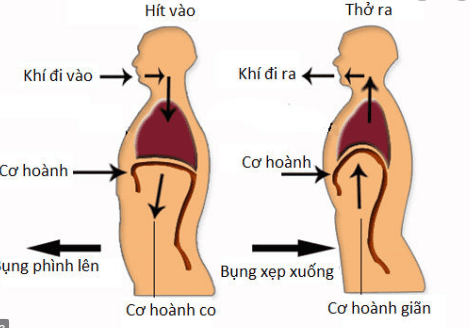
Hình 1: Cơ hoành ngăn cách khoang bụng với khoang ngực
The first case of diaphragmatic hernia was described in 1575 by Pare in a report of two autopsies of traumatic diaphragmatic hernias in adults.
The first report on hiatal hernia was published by Bowditch in 1853. In 1926, Akerlund suggested the term "diaphragmatic hiatus hernia".
In 1919, Angelo Soresi published the first report on elective surgical treatment of diaphragmatic hiatus hernia, entitled: "Horizontal hiatus hernia, frequency, diagnosis, basic surgical techniques". The purpose of this article is to call the surgeon's attention to hiatal hernias, especially small hiatal hernias, because patients who suffer from this condition are often treated inappropriately.
Following Soresi's report, many other techniques have evolved. Stuart Harrington et al. at the Mayo Clinic in 1928 reported the treatment experience of 27 cases, with a recurrence rate of 12.5%. This technique is mainly based on the technique of Soresi earlier, especially he emphasized: closing the hernia hole relieves symptoms, when the diaphragm cannot be closed, he will suture the hernia viscera to the abdominal wall. .
In 1970, Nissen's Angleplasty was quickly approved worldwide and became the most popular anti-reflux surgery. The original surgery was modified by Nissen and other surgeons. Closing the hernia is an essential part of anti-reflux surgery. Demeester and Johnson assessed that the most appropriate length of gastric coil is 2 cm, which is sufficient to significantly prevent reflux and reduce symptoms of dysphagia after surgery. It is a variation from Nissen 's surgery that is commonly used today .
Currently, there have been many studies in the world showing the effectiveness of surgery in the treatment of diaphragmatic hernia. These reports specialize in the study of treatment techniques for a certain type of diaphragmatic hernia. In particular, laparoscopic surgery in the treatment of diaphragmatic hernia has been proven by many authors around the world to be feasible, bring good results in terms of aesthetics, reduce postoperative pain and can be performed in Center with experience in laparoscopic surgery.
In Vietnam, many centers have successfully implemented endoscopic endoscopic treatment of diaphragmatic hernia.
2. Anatomy of the diaphragm
2.1 Structure of the diaphragm The diaphragm is a flat, broad muscular structure that separates the thoracic cavity from the abdominal cavity. Dome-shaped muscle, concave face toward abdomen. The diaphragm is composed of two parts: the fascia in the center and the muscular part at the periphery, so it is considered as a combination of many abdominal muscles. The diaphragm has many holes to let the organs, blood vessels and nerves go from the ribcage to the abdomen or vice versa from the abdomen to the chest. This is an important striated muscle because it plays a role in respiration.The muscular part of the diaphragm has three origins: the sternum, the flank, and the lumbar.
The sternum: the muscle fibers attach to the back of the sternum blade to form a bundle or two small bundles. This bundle together with the costal bundle (costal part) confines a slit called the sterno-costal cleft or the sternal-costal triangle, through which the superior epigastric vessels pass.
Ribs: The diaphragm is attached to the last six ribs by muscles. Some muscle strains attach to the costal cartilage and ribs VII, VIII, IX. Some children cling to ribs X, XI, XII.
Lumbar part: The diaphragm attaches to the lumbar spine by muscles and ligaments.
Right pillar: attaches to the body of the three (or four) upper lumbar vertebrae and the corresponding intervertebral discs. Left pillar: usually one vertebra higher than the right pillar, in the body and intervertebral disc of two (or three) upper lumbar vertebrae. On the medial border of each pillar is a band of fibers called the medial arch ligament.
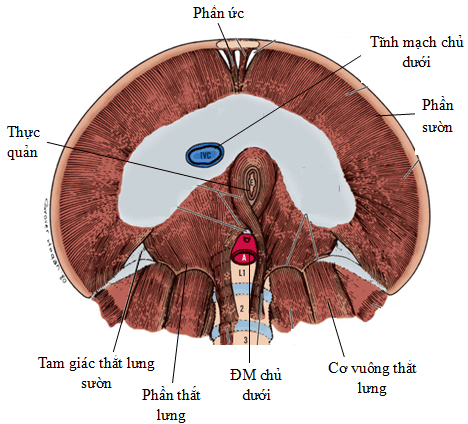
Hình 2: Cấu tạo cơ hoành (nhìn từ bên dưới) (Nguồn: Skandalakis LJ. (2006))
![Hình 3: Các lỗ của cơ hoành (thiết đồ đứng dọc) (Nguồn: Skandalakis LJ. (2006), [86])](/static/uploads/20200908_073127_168018_3_max_1800x1800_png_dd8bc29698.png)
Hình 3: Các lỗ của cơ hoành (thiết đồ đứng dọc) (Nguồn: Skandalakis LJ. (2006), [86])
The aortic fissure is the lowest and most posterior part of the diaphragm, close to the spine and located on the left edge of the midline, in a position relative to the body of the 12th thoracic vertebra.
The esophageal orifice is located in the muscular part of the muscle. diaphragm, corresponding to the 10th thoracic vertebrae, is formed by the muscles originating from the two right and left pillars, sometimes by the muscle fibers from the right column around the esophagus.
The esophageal foramen has 3 borders: the anterior and lateral borders of the hole are formed by the muscular arms of the diaphragm, and the posterior border is formed by the medial arch ligament.
Through a study of 50 human diaphragms, Botros et al. reported 5 different types of esophageal orifice.
2.3 Structure of the diaphragmatic pillars The right diaphragm originates from the anterior aspect of the first to fourth lumbar vertebrae, the left column originates from the first two or three lumbar vertebrae, from these intervertebral discs and anterior longitudinal ligament. The cylindrical fibers penetrate upward and anteriorly, forming the muscular arm that surrounds the opening of the aorta and esophagus. They then merge into the central tendon.
The forms of the diaphragm arm are very different. About 50% of the population of the right and left pillars originate from the right pillar. One third or so, the left arm originates from the right pillar and the right arm originates from both pillars.
Hernias of the diaphragmatic fissure are not associated with any particular cylindrical shape.
The foramen of the inferior vena cava of the diaphragm is located anteriorly and the highest of the three openings, corresponding to the body of the 8-9 thoracic vertebrae.
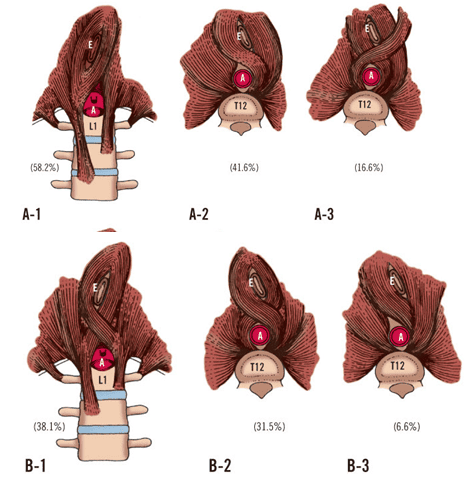
Hình 4: Các dạng phổ biến nhất của trụ cơ hoành (Nguồn: Skandalakis LJ. (2006))
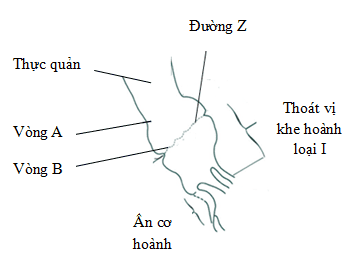
Hình 5: Sơ đồ minh họa vòng A và đường Z (Nguồn: . Peter J. Kahrilas (2008))
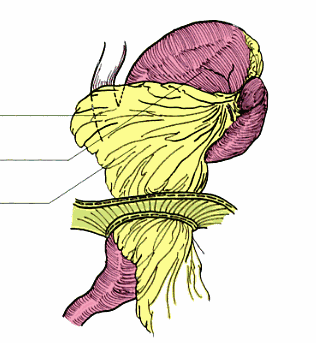
His angle function: creates a valve, preventing bile, stomach acid from backing up into the esophagus.
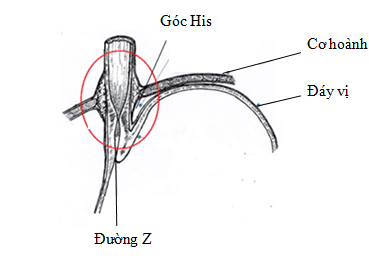
Hình 6: Cấu tạo của góc His (Nguồn: Peter J. Kahrilas (2008))
When the membrane of the esophagus - diaphragm is weak, or the esophageal slit is enlarged, the cardia will tend to herniate into the thorax.
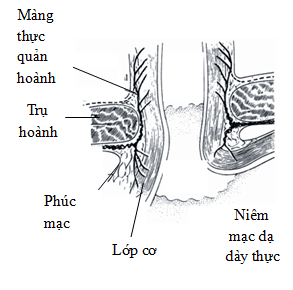
Hình 7: Cấu tạo màng thực quản - hoành (Nguồn: Skandalakis LJ. (2006))
When there is a hernia through the diaphragmatic fissure, the cardia moves upward, part or all of the lower sphincter is located in the thoracic cavity, negative intrathoracic pressure causes the resting tone of the lower sphincter to decrease. The upward displacement of the cardia causes the acute angle of His to cease to exist. These factors make reflux possible.
3. Hernia of the slit diaphragm
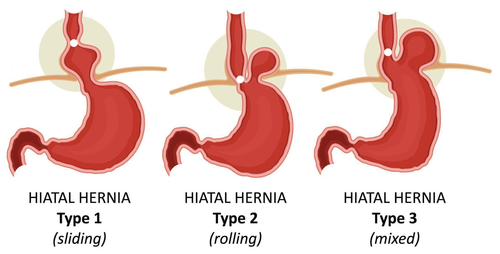
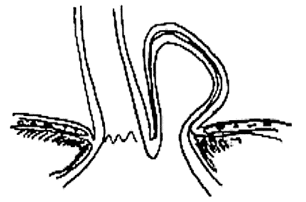
3.1 Definition Diaphragmatic hernia is a defect or opening in the diaphragm that allows abdominal organs to move into the chest cavity. A hiatal hernia occurs when the stomach or other organs protrude into the mediastinum through the esophageal opening of the diaphragm. 3.2 Classification of hiatal hernia Type I (also called sliding, concentric hernia) or axial hernia): With the esophageal junction the stomach slides into the mediastinum, pulling the stomach below it.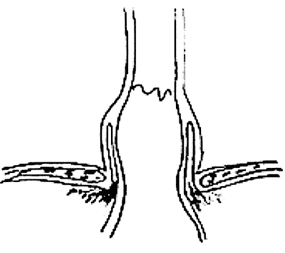
Hình 8: Thoát vị khe hoành loại I (Nguồn: Trus TL. (1997),)
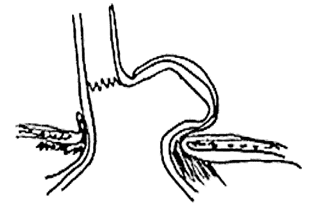
Hình 9: Thoát vị khe hoành loại II (Nguồn: Trus TL. (1997))
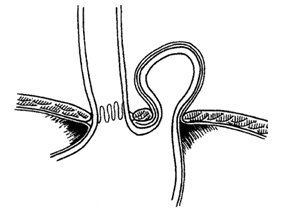
Hình 10: Thoát vị khe hoành loại III (Nguồn: Trus TL. (1997))
Type II, III, IV hernias are also called paraesophageal hernias.
Giant diaphragmatic hernia: depending on the definition of the authors, when the diameter of the hernia hole is larger than 5 cm [9], or more than 1/3 of the stomach is located in the thorax.
Hình 11: Thoát vị khe hoành loại IV khổng lồ (Nguồn: Jacques Perissat, (2004))
Hình 12: Thoát vị cạnh hoành
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.