
This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Nguyen Hung - Department of Medical Examination & Internal Medicine - Vinmec Danang International Hospital.Rhabdomyolysis is a condition in which the skeletal muscles are damaged, leading to the release of many toxins into the blood and the appearance of many dangerous complications such as: water and electrolyte disturbances, acid-base balance disorders, shock and serious The most important is acute renal failure due to myoglobin deposition in the renal tubules. So how to diagnose and treat acute renal failure due to rhabdomyolysis?
1. What is acute renal failure due to rhabdomyolysis?
Rhabdomyolysis is a condition in which damage to skeletal muscle fibers is caused by mechanisms such as:Direct trauma to skeletal muscle cells Acute rhabdomyolysis Intoxication also affects skeletal muscle. When skeletal muscle cells are damaged, broken will lead to the release of a series of substances into the circulatory system such as potassium, uric acid, myoglobin, lactic acid, creatine kinase (CK) enzymes... and lead to changes Symptoms such as:
Water and electrolyte disturbances Metabolic acidosis, hypovolemic shock, progressive acute respiratory failure (ARDS) and disseminated intravascular coagulation Most notably, acute renal failure due to rhabdomyolysis often appeared early, progressed rapidly.
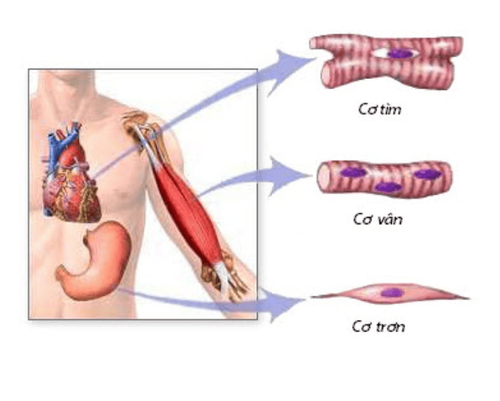
Tế bào cơ vân bị tổn thương sẽ dẫn đến hàng loạt biến chứng khác của cơ thể
Decrease in volume: The process of rhabdomyolysis causes extracellular fluid to be pulled into the cells and leads to hypovolemia. In addition, the contractile function of the heart muscle is also reduced due to toxicity, causing the kidney's filtration process to stop. Waste products from damaged skeletal muscle such as uric acid and myoglobin will be deposited in the renal tubules, hindering the filtering process of the kidneys and causing acute renal failure. The hypoperfusion of the body also affects the activity of renal tubular cells, contributing to acute renal failure due to rhabdomyolysis.
2. Risk factors for acute renal failure due to rhabdomyolysis
If the cause of rhabdomyolysis is a direct injury to the skeletal muscle cells accompanied by traumatic shock, the probability of acute renal failure rhabdomyolysis will be higher. The urine is red-brown and then turns black. signal the damage of the renal tubules due to the deposition of toxins from rhabdomyolysis and the presence of hemoglobin and myoglobin in the urine. Patients with low blood pressure, systolic blood pressure <90 mmHg will reduce blood supply to the kidneys, reduce glomerular filtration pressure and lead to acute renal failure due to rhabdomyolysis. Creatine Kinase >15,000 units/mL Acute respiratory failure. The length of time patients are diagnosed and treated is directly proportional to the risk of acute renal failure rhabdomyolysis, especially if treatment is delayed (> 12 hours).
Nước tiểu chuyển sang màu đen cho thấy tình trạng tổn thương nặng ở ống thận
3. Tests to help diagnose acute renal failure due to rhabdomyolysis
Urea and creatinine in the blood are elevated to help diagnose kidney failure. Elevated Creatine Kinase, typically >10,000 units/mL, especially >15,000 units/mL, is more likely to affect kidney function than uric acid, AST, ALT elevations Arterial blood gases suggest a condition respiratory failure and metabolic acidosis Electrolytes: decreased sodium, calcium and increased potassium and phosphorus. The higher the potassium in the blood, the higher the risk of heart arrhythmias. Tests for the cause of rhabdomyolysis Imaging: depending on the cause of the acute rhabdomyolysis.4. Treatment of acute renal failure due to rhabdomyolysis
General treatment The first thing to do is to ensure the first aid sequence according to the ABC principle: A (Airway): ensure airway clearance, B (Breathing): ensure respiratory failure, C (Circulation): ensure circulation in the body. The next step is to evaluate the degree of rhabdomyolysis, take temporary measures, and pay attention to the life-threatening condition such as cervical spine injury, traumatic brain injury... Find the cause cause rhabdomyolysis to solve, and at the same time treat complications that occur if any.
Đảm bảo trình tự cấp cứu bệnh nhân theo nguyên tắc ABC
Maintain systolic blood pressure above 90 mmHg with vasopressors such as dobutamine, dopamine, noradrenalin... in combination with fluid administration to restore intravascular volume. At that time, there are 2 possible cases:
If oliguria persists, urine volume is still less than 30ml/hour, intravenous furosemide loop diuretics should be used until urine volume is reached. 200ml/hour, maintain until rhabdomyolysis is resolved. On the contrary, if diuretics do not respond, it is necessary to appoint emergency dialysis to remove toxins from the patient's body, waiting for kidney function to recover. If the patient's urine volume is >50 mL/hour, administer Mannitol 20% 200 mL intravenously every 6 hours. If urine still does not increase, discontinue Mannitol and switch to a loop diuretic like Furosemide. Conversely, if the patient is responsive, with a urine volume greater than 200 mL/hr, treatment should be continued until risk factors for acute renal failure due to rhabdomyolysis have been resolved. Patients with acute rhabdomyolysis syndrome are at high risk for complications of acute renal failure if they experience symptoms such as red-brown urine, traumatic shock, measured systolic blood pressure less than 90 mm Hg, and symptoms. present acute respiratory failure or the patient is diagnosed with acute rhabdomyolysis and is treated more than 12 hours after the first symptoms of illness.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.













