This is an automatically translated article.
Posted by Doctor Vu Duy Dung - Department of General Internal Medicine - Vinmec Times City International Hospital
Myasthenia gravis (MG) is a well treatable disease with many effective treatments and with a natural course that is continuously improved by better diagnostic tests and therapeutic drugs effective. Diagnosing and treating patients with MG can be very rewarding for any neurologist because most patients can lead normal lives with proper treatment.
1. What is congenital myasthenic syndrome?
Congenital myasthenic syndromes are very rare hereditary neuromuscular diseases caused by pathological variations in genes encoding different neuromuscular-expressing proteins (Table 2). ). The most commonly implicated genes are those encoding AChR subunits (CHRNE, CHRNA1, CHRNB1, CHRND) and cause AChR deficiency or AChR kinetic dysfunction with functional deficiency or excess. Other commonly involved genes include several genes that encode proteins essential for terminal membrane development and function ( DOK7 , RAPSN , AGRN , LRP4 , MUSK ). COLQ mutations cause terminal membrane acetylcholinesterase deficiency; CHAT mutations cause a presynaptic congenital myasthenic syndrome due to acetyltransferase deficiency (Table 2).

Hội chứng nhược cơ bẩm sinh gây ra bởi các biến thể bệnh lý trong các gen mã hóa các protein khác nhau biểu lộ tại synap thần kinh-cơ
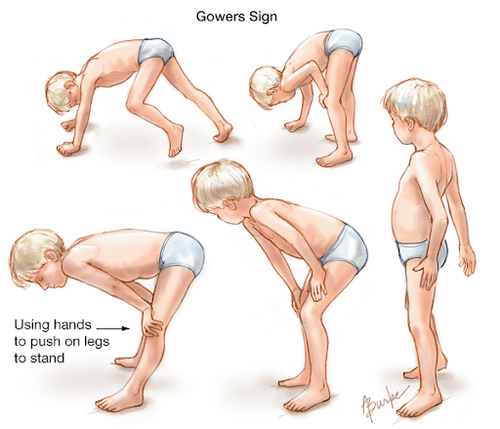
Congenital myasthenic syndromes are inherited in a dominant or recessive genotype, and the onset of symptoms is usually at birth or early infancy, and rarely in late infancy or childhood. early adulthood. The main clinical symptoms include skeletal muscle weakness in the ocular, medullary, limb, and respiratory muscles of different patterns and severity. In infants, symptoms include crying and weak suckling, respiratory distress, apnea, cyanosis, difficulty feeding, stridor, drooping eyelids, facial weakness, and sudden death. Later in childhood, developmental milestones can be delayed, and muscle weakness can cause fluctuating ptosis, difficulty running, and climbing stairs. Cardiac and smooth muscle are not affected, and cognitive function is normal in the majority of patients.
Table 2: The most common congenital myasthenic syndromes and their features
2. Diagnosis of congenital myasthenic syndrome
The primary differential diagnosis includes seronegative myasthenia gravis, congenital myopathies, and other causes of floppy infant syndrome.Certain clinical features are typical of certain types of congenital myasthenic syndromes and provide suggestive information to guide the diagnosis. For example, exacerbations and apneas caused by fever or agitation, family history of sudden infant death, and improvement over time are typical of congenital myasthenic syndrome with intermittent apnea. attacks (formerly known as familial myasthenia gravis) are caused by CHAT mutations. Congenital polyarticular stiffness, spasticity, flaccid infant syndrome, premature respiratory failure, and intermittent apnea occur in infants with congenital myasthenic syndrome caused by RAPSN defects. Stridor in infants, tongue atrophy, ptosis with preserved eye movement, facial features of myopathy, worsening with acetylcholinesterase inhibitors, and marked improvement with ephedrine or albuterol are typical features of impairment missing DOK7 .
Diagnosis is based on typical clinical features. These features include absence of serum AChR or MuSK antibodies; no typical signs of congenital myopathy on muscle biopsy; decrease in CMAP on low frequency repetitive nerve stimulation; Repeated CMAP after single stimulation (“dual response to single nerve stimulation” is typical of congenital slow ion channel myasthenia gravis and terminal membrane acetylcholinesterase deficiency/congenital myasthenia gravis syndrome. ); abnormal vibration on single fiber EMG; no clinical response to plasmapheresis or other immunosuppressive agents; a positive response to acetylcholinesterase in most but not all cases; and identified a defect in one of the genes known to cause a congenital myasthenic syndrome . Genetic testing may begin with single-gene testing in cases with features typical of a particular congenital myasthenic syndrome, or multi-gene or whole-genome testing in less clinically suggestive cases. typical sieve. A list of most pathologic genes in congenital myasthenic syndromes is available on the market for testing.

Xét nghiệm gen có thể chẩn đoán hội chứng nhược cơ bẩm sinh
Treatment with acetylcholinesterase inhibitors (pyridostigmine and 3,4-diaminopyridine) is effective in most cases of myasthenic syndrome with the exception of DOK7 and slow channel myasthenic syndrome. Albuterol and ephedrine are very effective in congenital myasthenic syndrome with DOK7 and COLQ defects. Fluoxetine is beneficial in some patients with slow-channel congenital myasthenia gravis.
Thuốc ức chế acetylcholinesterase có hiệu quả trong điều trị hội chứng nhược cơ bẩm sinh
CONCLUSION
Congenital myasthenic syndromes are very rare diseases that need to be distinguished from autoimmune forms of neuromuscular synaptic diseases because treatment can be very effective.
Source:
Emma Ciafaloni. Myasthenia Gravis and Congenital Myasthenic Syndromes. Continuum (Minneap Minn) 2019; 25 (6, Muscle and Neuromuscular Junction Disorders):1767-1784.