This is an automatically translated article.
The article was written by MSc Nguyen Thi Hang - Laboratory Doctor, Laboratory Department - Vinmec Times City International General HospitalImmediate biopsy, also known as frozen section (FS) is a histopathological technique that allows rapid microscopic analysis/diagnosis right in surgery, helping the surgeon orient and decide on the appropriate surgical strategy.
1. What is an Immediate Biopsy?
Immediate biopsies have been used as a method of hardening tissue samples for fragmentation since 1818. Immediate biopsies were first used for intraoperative diagnosis by Welch on surgical breast tumors by Halstead at Johns Hopkins (Baltimor, Md) in 1982. By the 1960s, when cryostat was first introduced, immediate biopsies had become a routine part of the diagnostic protocol (1).Today, this technique is widely applied, routine, widespread worldwide and is a commonly used technique in cancer surgery.
2. In what cases is immediate biopsy indicated?
Immediate biopsy is used in the following situations: Provides rapid macro and microscopic diagnosis to identify unknown pathological conditions, allows the diagnosis of tissue samples as benign or malignant, or identifies spread of the disease, assess the cut area, the distance from the tumor area to the surgical cut area is safe enough, to detect metastasis or simply to determine the nature of the tissue sample. The histological procedure provides an appropriate and accurate diagnosis, prognosis, and allows special tests to be performed. To confirm the final tissue sample, the diagnosis should be performed on a routine tissue sample. Do not use immediate biopsy if: The diagnosis of cryosection does not have an immediate effect on decision making. Tissue samples need to be permanently transferred (either because they are single or small or require extensive testing). Consider not using an immediate biopsy if: The cryosection is known to cause serious sham changes that affect decision making. The tissue sample is highly calcified. High risk of infection. The specimen is adipose tissue.
Kỹ thuật sinh thiết tức thì thường được sử dụng trong phẫu thuật ung thư
3. How is an Immediate Biopsy performed?
Tissue specimens will be sent to the pathology laboratory right within the surgery. Samples submitted must be fresh samples, not fixed.At the laboratory, the pathologist will select the areas of the lesion that need cryosection, take a representative of this lesion or, if the submitted sample has been selected by the surgeon, will be moved directly to the next technical step.
The pathologist will bury the tissue sample in cryostat at -200C to -150C and use a special cutter to cut the frozen tissue into thin slices.
The thin section of this tissue sample is then stained with hematoxylin-eosin to bring out the colors of different cell components.
Next, this stained tissue section will be evaluated by the pathologist and diagnosed immediately during surgery.
Results will be notified directly by the pathologist by phone to the surgeon.
The whole procedure from the time the specimen is removed from the body, to the time the surgeon receives the answer, is done within up to 30 minutes.
The remaining cold cut tissue sample will then be fixed in 10% neutral formalin solution and undergo routine histological block transfer procedure.
Sometimes in some cases, the pathologist will do more cytology techniques, to perform cytological diagnosis in parallel with cryosection of the surgical sample to help support the diagnosis. fast in surgery. Intraoperative cytology was also performed routinely. Combining these two methods will increase the sensitivity and specificity of the immediate biopsy diagnosis (2) (3).

Mẫu bệnh phẩm mô sẽ được gửi đến phòng xét nghiệm giải phẫu bệnh ngay trong cuộc mổ
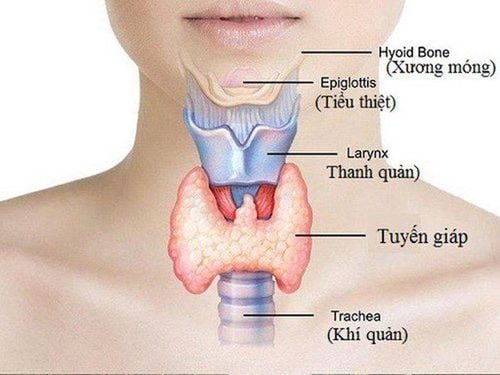
4. Can an Immediate Biopsy Detect Thyroid Cancer?
Thyroid nodules are a common finding in the population. Most of these nodules are benign, while 5-20% are malignant. The cytological diagnosis of samples obtained from fine needle aspiration FNA has been widely applied as a diagnostic method, changing the diagnostic and therapeutic approach to thyroid nodules.The main role of cytology is to distinguish positive cases from malignant cells (when surgery is indicated) from negative cases. Diagnostic cytology provides valuable information for the pathologist during the intraoperative consultation. Because of the high cytological accuracy, the value of immediate biopsies for thyroid nodules has become a matter of controversy.
This occurs because of the accuracy of cytological diagnosis with papillary carcinoma and the low sensitivity of immediate biopsy diagnosis for follicular lesions. However, immediate biopsies are still a very useful procedure, and pathologists are still frequently required to use them (3).
Does immediate biopsy help diagnose the nature of the thyroid nodule as benign or malignant? Immediate biopsies are not indicated for diagnostic purposes of the lesional nature of most thyroid nodules; the frequency of indications for FS is decreasing for purposes of determining the nature of the lesion. The diagnostic results of an immediate biopsy may contradict the diagnosis of FNA. Some cases of highly differentiated carcinoma cannot be diagnosed by immediate biopsy.
Some limitations of immediate surgical biopsy of thyroid gland (5) (3):
False negatives: For minimally invasive follicular carcinoma:
Sensitivity ranges from 17- 42% ( Presse Med 2008;37:949) It takes an average of 9 candle blocks to determine vascular intrusiveness ( Am J Clin Pathol 2001;115:370 ). Most diagnoses of 'cystic lesions' are diagnoses that need to be made on routine histological resections. False positive: Metastatic papillary carcinoma: in fact, the metastasis is actually Riedel's thyroiditis, diffuse hyperplasia, or ectopic thyroid tissue. Artificial transformation by cryosection may confuse the nuclei of papillary thyroid carcinomas with parathyroid neoplasms (Thyroid 2008;18:419). Post-FNA changes can be mistaken as cortical or vascular infiltrates on the diagnostic piece. In fact, the technique of fine needle aspiration (FNA) is a preoperative diagnostic method with high accuracy, used to diagnose thyroid nodules in detecting cancer. However, fine needle aspiration cytology has certain limitations.
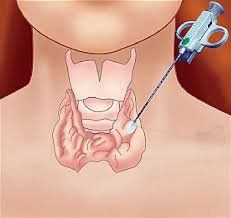
Thực tế cho thấy kỹ thuật chọc hút kim nhỏ tuyến giáp là phương pháp chẩn đoán có độ chính xác cao
Does an immediate biopsy help the surgeon navigate the surgical approach? The answer is yes. The role of an immediate biopsy is to provide a rapid diagnosis, allowing the surgeon to make immediate decisions during surgery. It helps to assist in cases where the thyroid nodule has a cytological diagnosis of undetermined and when an immediate biopsy reveals malignancy, it allows the surgeon to perform immediate thyroidectomy. avoids a second surgery for contralateral nodule resection - increased risk of disease transmission, increased mortality and complications (6).
In contrast, in some cases where cells are classified as benign Bethesda II, the diagnosis of cryosection can replace surgical management from extensive, invasive surgery down to conservative surgery (4).
Immediate biopsy of the thyroid gland allows : 1) confirm the diagnosis by cytology; 2) Diagnosis of suspected nuclei for which diagnostic cytology is undetermined; 3) identify the mass during surgery; 4) determine the extent of tumor penetration beyond the armor sheath or not; 5) Examine regional lymph nodes to determine the presence of metastases (4).
For cystic lesions, limitations exist in both cytological diagnosis and immediate biopsy, but combining the two methods of analysis increases the diagnostic level of immediate biopsy .
Immediate biopsy had a higher diagnostic accuracy than FNA cytology for the thyroid nodules classified as Bethesda II, III and IV (p<0.05). However, the diagnostic accuracy of FNA was markedly higher for patients classified as Bethesda V and VI than with immediate biopsy (p < 0.05) (4) (5).
Therefore, although the role of immediate biopsy for thyroid nodules is increasingly narrowing due to the high diagnostic value of FNA cytology, immediate biopsy still shows certain values. its in surgery. Therefore, this is still a useful and frequently requested method by pathologists and surgeons.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
Articles source:Raja Jouini, Nihed Abdessayed*, Wafa Koubba-Mahjoub, Ehsen ben Brahim and Achraf Chadli Debbiche. The Value of Intra-Operative Frozen Section in Thyroid Neoplasm: Management: Experience of One Center. s.l. : Jouini et al., Thyroid Disorders Ther, 2017. Richard M. DeMay, MD. Frozen Section of Thyroid? Just Say No. s.l. : Am J Clin Pathol: 110: 423-424, 1998. Jing Huang, Jieli Luo, Jianshe Chen, Yang Sun, Chao Zhang, Kanlun Xu, Qin Ye & Pintong Huang. Intraoperative frozen section can be reduced in thyroid nodules classified as Bethesda categories V and VI. s.l. : Scientific Reports volume 7, Article number: 5244 , 2017. Patol, Theresinha C. Fonseca1 Ana Suyia A. Eisenberg1 Mário Vuiio C. Araújo Jr.1 J. Bras. Accuracy of intraoperative consultation in thyroid nodules: analysis of 2040 cases performed at Institution National Cancer in 12 years. s.l. : Med. Lab. vol.51 no.5 Rio de Janeiro Sept./Oct. 2015, 2015. Bahadir Cetin, Sabahattin Aslan, Celal Hatiboglu, Bahattin Babacan. Frozen section in thyroid surgery: Is it a necessity? s.l. : Canadian journal of surgery. Journal canadien de chirurgie 47(1):29-33, Source, PubMed, 2004. https://www.pathologyoutlines.com/topic/methodsfrozen.html https://www.pathologyoutlines.com/topic/thyroidfrozen.html