This is an automatically translated article.
Surgical ligation of the ductus arteriosus is indicated for cases of failed drug closure treatment or small, medium, and calcium-free ductal arteriosus... The technique of ductal ligation should be performed properly. Standardized by a cardiologist.
1. Learn about the ductus arteriosus
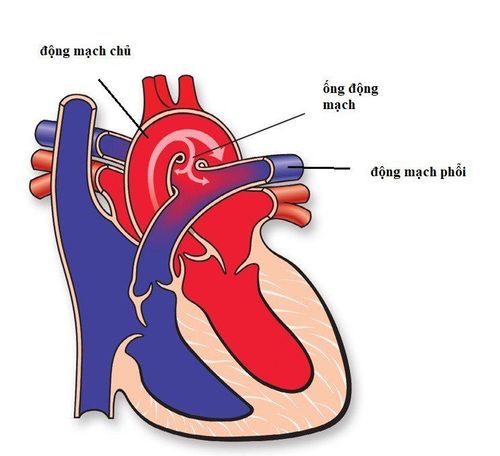
The ductus arteriosus begins to develop from the 6th week of pregnancy. This is the main drainage route of the right ventricle (because the lungs are not yet functioning). Usually, the ductus arteriosus closes 12 hours after birth (in full-term infants) and completely closes by 2 to 3 weeks of age.
The ductus arteriosus is the part that usually connects the superior part of the descending aorta (about 5-10mm from the origin of the left subclavian artery) and the proximal left pulmonary artery. This organ is usually cone-shaped, the tip on the lung side is smaller. The ductus arteriosus can be long or short, straight or tortuous. There may be bilateral ductus arteriosus.
Simple ductus arteriosus accounts for 5-10% of all congenital heart disease cases, male/female ratio is 1:3, the disease is more common in premature and low birth weight infants.
The degree of ductus arteriosus is classified as follows:
Small ductus arteriosus: Tube diameter < 1.5mm, no signs of left heart overload; Medium ductus arteriosus: Tube diameter 1.5 - 3mm, with signs of mild and moderate overload of the left heart; Large ductus arteriosus: Diameter > 3mm, left heart is severely overloaded.
2. Indications and contraindications for ductal ligation surgery
2.1 Designation
Premature babies, low birth weight, failed treatment of closure of the ductus arteriosus with ibuprofen or indomethacin; Neonatal ductus arteriosus, medium or small ductus arteriosus; The ductus arteriosus is soft, without calcium.
2.2 Contraindications
Patients with large ductus arteriosus, cyanosis due to right-left shunt, cardiac catheterization with pulmonary vascular resistance > 8U/m2, unresponsive to oxygen, NO and other pulmonary vasodilators; People with duct-dependent congenital heart disease.

Người bị bệnh tim bẩm sinh không được thực hiện phẫu thuật mạch máu
3. The surgical procedure for ligation of the ductus arteriosus
3.1 Preparation
Diagnose the patient's disease; Conduct consultation before surgery; Perform necessary tests for closed heart surgery; Re-examine the patient 1 day before surgery; Endotracheal anesthesia in the operating room, central venous catheterization, invasive artery placement, epidural analgesia (it is better to relieve pain for patients than to remove the tube soon after surgery or remove the tube right in the operating room) ; Place the patient in the right side lying position.
3.2 Technical implementation
Have the patient lie on the right side; The left posterior skin incision follows the curve, about 1-2cm below the top of the scapula, the incision passes through the lower part of the scapula, between the lower border of the scapula and the spine; Enter the left chest through the 3 - 4 intercostal space in the pleura (or extrapleurally in neonates); Dissection clearly reveals descending aorta and ductus arteriosus, taking care not to injure the lymphatic ducts and recurrent laryngeal nerve. At the same time, the waist and aortic arch should be checked before performing a ductal ligation; Use forceps to temporarily clamp the ductus arteriosus before ligation; Ligation of the ductus arteriosus with 2 threads at the head of the lung and the head of the aorta, sewn into the outer layer before ligation; In case of necessity, the third thread can be used to tie between the two threads; After ligation of the ductus arteriosus, suture of the mediastinal pleura was performed. In the case of going in the pleura, a pleural drainage is placed in the intercostal space 6-7 in the middle axillary line, aspirating negative pressure of 20cm of water.
3.3 Risk of complications
Surgical ligation of the ductus arteriosus has a number of potential risks such as:
Residual shunt after tubal ligation intervention; Pseudobulbular mass is rare after ligation of the ductus arteriosus; Paralysis of the phrenic nerve; Paralysis of the left recurrent laryngeal nerve; Pleural emphysema. Depending on the case, the doctor will have the appropriate treatment intervention.
When being indicated for ductal ligation surgery, the patient should absolutely follow all instructions of the doctor to ensure the successful treatment process and minimize the risk of risks.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.