This is an automatically translated article.
The article was written by Gastroenterology specialist, Department of General Surgery - Vinmec Times City International Hospital.
Appendicitis is a common surgical emergency in gastrointestinal emergencies. Appendicitis usually occurs in men, the most common age: 15-40 years old. The male/female ratio is about 1.3:1. Appendicitis is common, easy to diagnose but often leaves serious complications if not properly diagnosed and treated early with standard surgery within 24 hours of the onset of pain.
1. How dangerous is appendicitis?
When the appendix is acutely inflamed, it usually bursts with pus after 24 hours. In some patients, the appendix may rupture after 12 hours. There is a case where the appendix burst pus after 6 hours from the time the patient started the pain. In clinical practice, it is impossible to predict when acute appendicitis will rupture.
If the disease is delayed, it will develop in many ways without predicting its course. Complications are peritonitis, intra-abdominal abscess or appendicitis... Complications from untreated appendicitis bring a lot of trouble to the patient, even leading to death. mortality (death rate ranges from 0.2 to 0.8%). The prognosis of a patient with acute appendicitis depends on several factors: clinical form of appendicitis, age of the patient, comorbid medical conditions...
Chronic appendicitis is a Rare pathology of the appendix, the onset is acute appendicitis followed by remission. The cause is that the lumen of the appendix becomes blocked and then re-opens on its own, and this phenomenon can be repeated many times.
Common causes of the disease are:
Obstruction of the appendix lumen due to stones, feces, worms, flukes, tumors, may also be due to hyperplasia of the lymph nodes. Inflammatory lesions caused by ulcers in the mucosa cause bacterial infection in the wall of the appendix. Common pathogens in appendicitis are E.coli, Bacteroides fragilis.

2. Points to note about appendicitis
Appendicitis accounts for a large frequency of abdominal emergencies (about 30%) so a patient presenting to the hospital with abdominal pain, especially pain in the right iliac fossa, must first be checked for appendicitis. or not. For cases that are difficult to monitor for many hours, repeat the examination many times to avoid missing out. Early, correct diagnosis and surgical intervention within the first 24 hours of pain minimize the complications and complications of appendicitis.
3. Symptoms of appendicitis
3.1. Functional symptoms Dull pain localized in the right iliac fossa. This is a typical symptom of appendicitis. Anorexia almost always accompanies appendicitis. Nausea or vomiting occurs only in about 75% of patients, vomiting symptoms are not specific. 3.2. Body symptoms Fatigue, lethargy Fever: the temperature is sometimes not high, only 37.3 degrees Celsius - 38 degrees Celsius Infection face, dry lips, dirty tongue, bad breath. 3.3. Physical symptoms The most common sign on abdominal examination is tenderness in the lower right quadrant of the abdomen or in the triangle of the appendix, which is the appendix located in its most common location. Press the abdomen in the following locations:
Pain point in the third outside the line between the navel and the right anterior superior iliac spine (Mc Burney point) The pain point at the intersection of the line between the navel and the right superior anterior iliac spine with the border outside the rectus muscle (Clado point) Pain on the right lateral third of the anterior superior iliac interspinous junction (Lanz point) Signs of muscle tension in this area (abdominal wall response) on pressure, if present, have a high value in diagnosis.
4. Subclinical
Complete blood count : increased white blood cell count, especially neutrophils. Abdominal ultrasound: showing an enlarged appendix or infiltration of fat - fluid around the appendix. The definitive diagnosis of acute appendicitis by ultrasound has a sensitivity of 78-85% and a specificity of 80-95%. Abdominal X-ray: is of little value in diagnosing appendicitis but very valuable in detecting comorbidities such as gastric perforation - intestinal obstruction. Computerized tomography of the abdomen: rarely used due to its high cost, applied only to difficult cases. However, it is an effective tool for diagnosing appendicitis as well as for differentiating. with pelvic inflammatory disease and pelvic inflammatory disease. Laparoscopy: this is a method for both diagnosis and treatment. Laparoscopy is perhaps most useful for evaluation in women with lower abdominal pain.

5. Diagnosis
Definitive diagnosis
Diagnosis of appendicitis is usually based on the following symptoms: localized dull abdominal pain in the right iliac fossa, fever, signs of infection
Physical symptoms: tenderness in the pelvic fossa must have abdominal wall reaction
Subclinical: elevated white blood cell count, ultrasound image of enlarged appendix (or abdominal computed tomography results for appendicitis).
However, in some cases the symptoms are not necessarily typical and complete.
6. Some special forms of acute appendicitis
6.1. Appendicitis in children: Often more difficult to diagnose than adults (or with gastrointestinal disorders), the process is rapid, the appendix ruptures, causing peritonitis.
6.2. Appendicitis in the elderly: 2 common clinical forms in the elderly are:
Semi-obstruction Intestinal tumor. The frequency of appendicitis in the elderly is lower but there are many serious complications with accompanying pathological complications such as heart, lung....
6.3. Appendicitis in pregnancy Appendicitis is the most common extrauterine disease that requires surgical treatment during pregnancy. The frequency is approximately 1/2000 pregnancies. Acute appendicitis can occur at any time during pregnancy, but is most common during the first two trimesters. As the fetus grows, the diagnosis of appendicitis becomes more and more difficult because the appendix is displaced upward and outward.
Surgery during pregnancy will have a risk of preterm birth from 10-15%. The most important factor associated with maternal and fetal mortality is appendicitis perforation or appendicitis peritonitis. Fetal mortality in early appendicitis is 3-5%, which increases to 20% when appendicitis is perforated or peritonitis occurs. Appendicitis during pregnancy is prone to many complications for mother and child, so it is necessary to diagnose quickly and intervene early.
7. Appendicitis Treatment
Surgical intervention by open surgery or laparoscopic surgery (robot surgery, laparoscopic single incision or laparoscopic surgery through natural opening) early when appendicitis is diagnosed. The sooner the better. This is the classic treatment and is accepted by all clinicians worldwide ever since.
From 2004 to now, there have been a number of studies on non-operative treatment of uncomplicated appendicitis with antibiotics. The results from these studies show that the success rate of antibiotic treatment for uncomplicated appendicitis is 90% (as seen in cases of bacterial appendicitis, the patient comes from a very early stage). , 10% did not respond and had complications requiring surgical intervention.
Follow-up of patients who successfully treated for uncomplicated appendicitis within 1 year had 30% of recurrent appendicitis, so treatment of uncomplicated appendicitis with antibiotics cannot definitively cure enteritis. excess and the disease will have a very high risk of recurrence in a short time, in addition in these studies the sample size is not large enough compared to the worldwide prevalence.
Therefore, the gold standard of treatment for appendicitis remains surgical removal of the inflamed appendix. This is an effective method to help definitively treat appendicitis. The treatment of appendicitis with antibiotics must be selected and considered carefully for each patient and must be approved by the home management agency. water
Open appendectomy
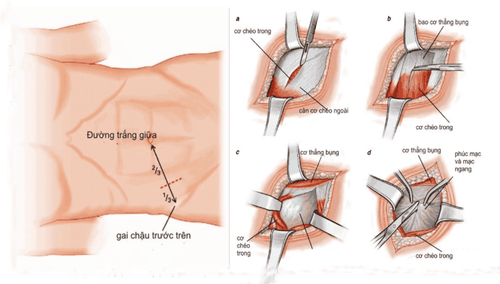
After the patient is anesthetized, disinfect the abdominal wall with an antiseptic solution and spread a sterile cloth, exposing the right lower right quadrant of the abdomen. Cut the skin diagonally at right angles to the line connecting the anterior superior iliac spine and the umbilicus, about 2-3 cm from the superior anterior iliac spine (Mc Burney line), cut the great diagonal fascia and separate the muscle into the peritoneal cavity to expose the appendix.

Expose the appendix: cut the mesenteric appendix (appendiceal artery) suture the hemostasis. Treatment of the appendix root: the appendix stump is the convergence of 3 longitudinal muscle bands of the cecum, the appendix root is tied or sutured. closed with criteria , can be included or not included Wipe the abdominal cavity, check Meckel's diverticulum, cut the area of the mesentery and the appendectomy to treat the lesions (if any), send appendiceal specimens as tissue pathology Suture to restore muscle fascia, suture skin. Laparoscopic surgery is the method of first choice for appendectomy in all cases unless there are contraindications to laparoscopic surgery such as patients with severe cardiovascular or respiratory disease unable to tolerate surgery. laparoscopic surgery, or patients with a history of previous laparotomy many times... Laparoscopic surgery is most commonly used in the treatment of appendicitis because of its many outstanding advantages. These can be mentioned as faster recovery time, less pain, small incisions, especially good for people with thick abdominal wall.
Laparoscopic appendectomy has been widely applied since the 1990s, including traditional laparoscopic surgery or modifications such as: single-incision laparoscopic surgery (SILS), laparoscopic automatic perforation. natural or laparoscopic surgery using robotic (robotic) arms. No matter which method is used, it must ensure the following principles: clean the abdomen, remove the appendix, well handle the appendix root, the mesentery.
In case the appendix is difficult to perform well and safely with laparoscopic surgery, it will be converted to open surgery. It's not a failure with laparoscopic surgery, it's just about changing the treatment to make it safer for the patient.
The basic steps of laparoscopic appendectomy are:
Prepare the patient well before surgery, ensure adequate hydration, electrolytes, and preoperative cardiopulmonary examination.
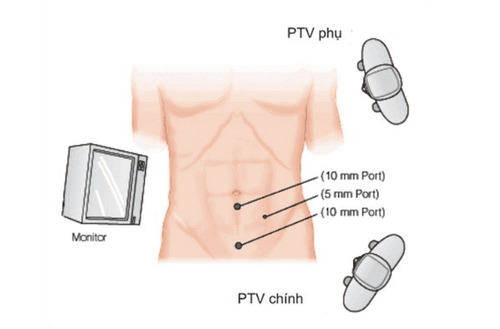
The patient is anesthetized, lying on his back, arms folded along his body. The main surgeon stands on the left side of the patient, the assistant (holding the camera) stands on the same side as the main surgeon and near the patient's shoulder. Monitor is located on the right side.
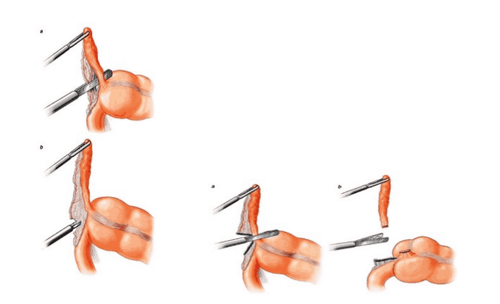
Expose the appendix: Cut the mesenteric appendix (appendiceal artery) with bipolar electric knife (bipolar) Treatment of the appendix root: the base of the appendix is the convergence of 3 longitudinal muscle bands of the cecum, the base of the appendix tied or sutured with staples that can be clipped Clips with buckles in some cases can be managed with a laparoscopic stapler Clean the abdomen, examine Meckel's diverticulum, mesenteric section and apex. appendectomy to treat lesions (if any), remove appendix for histopathology. Stitching to restore the trocar holes, suturing the skin Using antibiotics to treat after surgery. Postoperative care after surgery: 12 hours after surgery, the patient can have a light meal, exercise gently in place, change the wound dressing daily, the patient can be discharged from the hospital 3-5 days after surgery.
Appendicitis is a common abdominal surgical emergency that needs to be examined, properly diagnosed and treated early. For difficult cases, they need to be examined and monitored regularly at the hospital.
Inflammatory appendectomy is the gold standard for treatment, laparoscopic surgery is the first choice, but when facing difficult cases, surgeons should switch to open surgery to ensure the goal. safest for the patient.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of doctors, modern equipment and technology, but also stands out for its examination, consulting and service services. comprehensive and professional medical treatment; civilized, polite, safe and sterile medical examination and treatment space.
If you have a need for consultation and examination at Vinmec Hospitals under the national health system, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.