This is an automatically translated article.
The article was written by MSc Nguyen Van Huy - Emergency Medicine Doctor, Emergency Department - Vinmec Ha Long International HospitalAcute adrenal insufficiency (STTC) is a medical emergency due to acute deficiency of corticosteroids (cortisol, aldosterone). Diagnosis is often difficult due to nonspecific clinical and biological symptoms. The diagnosis is more favorable if considered, as it is one of the leading causes of death, the disease is often missed with the diagnosis of cardiovascular collapse of unknown cause. Therefore, it is necessary to be treated promptly and on the spot even when the diagnosis has not been confirmed, with only a few suspicious symptoms.
1. Predisposing factors of acute adrenal insufficiency
Infections, especially sepsis caused by blue pus bacilli, meningococcal, adrenal gland surgery Adrenal hemorrhage After anticoagulation/Coagulation disorders Abrupt cessation of corticosteroids, adrenal suppressing drugs Adrenal neoplasms, other metastatic tumors
2. Anatomical features of the adrenal gland
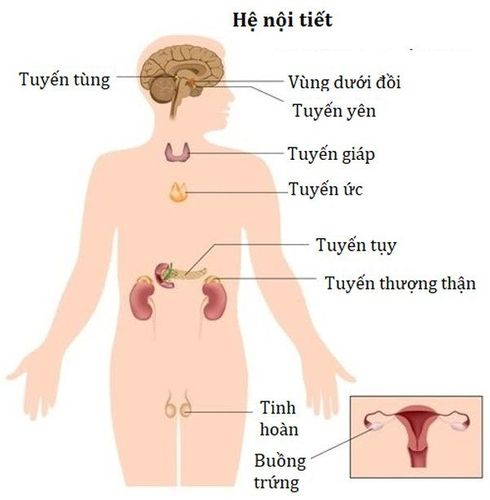
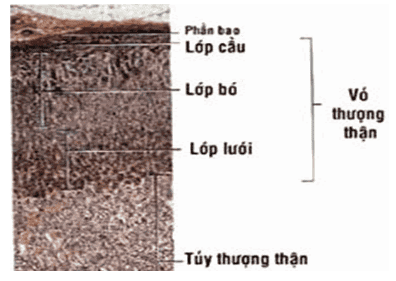
The adrenal gland consists of two small glands located on top of the kidneys, each weighing about 4g. The adrenal gland consists of two distinct parts: the cortex (80%) and the medulla (20%).
Adrenal cortex: Consists of 3 separate layers
The globular layer consists of very thin cells located on the outermost layer of the gland, producing the mineralocorticoid mineralocorticoid (aldosterone) hormone that metabolizes water and salt. The middle bundle layer produces glucocorticoids (cortisol). The inner reticulum secretes androgens.
3. Diagnosis of acute adrenal insufficiency
3.1 Clinical
Digestive disorders: epigastric pain, then spread to the whole abdomen, but the abdomen is still soft, sometimes accompanied by nausea and vomiting. The above manifestations can be confused with a surgical abdominal pathology. Psychiatric disturbances with fatigue to coma, or vice versa excitability, delirium, confusion. Cardiovascular collapse, rapid drop in blood pressure, cold hands and feet, small, fast pulse. Signs of extracellular dehydration include weight loss, muscle pain, and sometimes fever, even though there are no signs of infection. In addition, it can be associated with widespread pain such as myalgia, arthralgia, headache, and other signs of predisposing factors such as infection, musculoskeletal disease...etc.
3.2 Subclinical
Blood electrolyte disorders: Decreased sodium, decreased chlorine, increased potassium due to Aldosteron deficiency, decreased blood glucose due to Cortisol deficiency. Blood protein increased, Hct increased due to loss of circulating fluid due to lack of Aldosterone (salt-water reserve). Quantitative blood cortisol 8h-20h showed a decrease. Normally, cortisol rises when you wake up in the morning, and lowers when you go to sleep at night. In addition, there may be: eosinophilia, hypercalcemia (6%), acidosis, anemia. Are the factors that promote or accompany. If the amount of ACTH is elevated, it means primary adrenal insufficiency (adrenal origin), if ACTH decreases or the ACTH test increases blood cortisol, it is secondary acute adrenal insufficiency (due to non-pituitary failure). can produce ACTH, so it cannot command the adrenal glands to secrete Cortisol).
3.3 Factors supporting the diagnosis
Darkening of the skin (suspected Addison's disease) Cushing's syndrome
3.4 Differential diagnosis
Shock hypovolemic due to dehydration, blood loss Cardiac shock Infectious shock
4. Causes of acute adrenal insufficiency
STTC can occur in the setting of primary (in the adrenal gland) or secondary (below the hypothalamic-pituitary gland).
4.1 Adrenal causes
On the adrenal gland, lesions of the adrenal gland can be the manifestation of a primary schizophrenia, regardless of the cause. Factors predisposing to STTC such as:
Infection, surgery, vomiting. Take a laxative, antidiarrheal, or diuretic. Sweat a lot, eat a lot and last for a long time. Quit hormone replacement therapy. Bilateral adrenal haemorrhage Bilateral adrenal haemorrhage and hemangioma are rare, severe lesions that are often detected at autopsy. Non-traumatic adrenal haemorrhage is usually due to coagulopathy. May be due to disseminated intravascular coagulation or coagulation diseases (cancer, blood diseases), but most commonly due to anticoagulant therapy.
Bilateral adrenal hemorrhage can also occur from anti-adrenal therapy with OP'DDD [2,2 bis-(2-chlorophenyl, 4-chlorophenyl)-1,1-dichloroethane].
In children with Waterhouse-Friderichsen syndrome, perinatal bilateral adrenal haemorrhage causing acute adrenal insufficiency is often due to successive vascular collapse due to blood loss.
Congenital disorders of adrenal hormone synthesis Very rare, seen only in pediatrics, it is a condition of salt loss in infants with 21-hydroxylase blockade. The disease appears days to weeks after birth with anorexia, no weight gain, vomiting, dehydration, and cardiovascular collapse. Death in the setting of acute adrenal insufficiency if not treated properly and promptly. Children urinate a lot of sodium even though the blood sodium is reduced, with a decrease in blood chloride and an increase in blood potassium. In female children, there is often an abnormality of the external genitalia. Other enzymes, much rarer also, also cause salt loss syndrome, eg 11-hydroxylase deficiency, 3.(-ol-deshydrogenase or more rarely: 20-22 desmolase

Sử dụng thuốc nhuận tràng là yếu tố làm xuất hiện STTC
4.2 Other causes
OP' DDD not only inhibits the synthesis of Cortisol but also has anti-mitotic effects that cause adrenal atrophy. Aminoglutethimide is another synthetic anti-adrenal agent that inhibits cortisol synthesis with a risk of adrenal insufficiency from the first days of therapy. Some cases of acute adrenal insufficiency caused by continuous high-dose ketoconazole treatment. Rifampicin is a liver enzyme inducer that increases the oxidation of cortisol to 6-bhydroxycortisol. Some other enzyme inducers such as Gardenal, Dihydan (phenitoin). Other rarer causes include cholesterol embolism, thrombosis of an adrenal artery or vein, and fungal infection (cryptococcose). Total adrenalectomy, requiring hormone replacement therapy.
4.3 Hypothalamic-pituitary causes
Surgery for anterior pituitary adenoma. Sheehan's syndrome. Injury. Meningitis . Aneurysm rupture of an internal carotid artery. Hemorrhage of the pituitary gland (hemorrhage of the pituitary gland). The Metyrapone test can lead to STTC, especially towards the end of the test. Surgery to remove an adrenal gland due to a tumor. Occurs due to abrupt discontinuation of therapy after a prolonged course of corticosteroids.
5. Treatment of acute adrenal insufficiency
5.1 Emergency
First 24 hours
Place an intravenous line with a large needle Get blood for testing. Rapid infusion of 2-3 liters of 0.9% NaCl or 0.9%/G 5% NaCl (according to hypovolemia, CVP, hemodynamic parameters if possible, electrolytes, blood sugar) IV immediately 100 mg Hydrocortisone then continue 100 mg / every 6 hours
Use supportive measures (if necessary) if the patient is in severe shock, coma, respiratory or circulatory failure. Treatment follows three main directions: adjustment of water, electrolytes, hormone replacement. Regular clinical and paraclinical follow-up.

24 giờ đầu nên tiêm tĩnh mạch
5.2 Measures to stabilize the patient
Continue infusion of 0.9% NaCl at a slower rate for the next 24-48 hours Find and treat the trigger Perform the ACTH test to confirm the diagnosis Find the cause of the adrenal insufficiency Reduce the dose of hydrocortisone gradually in 1-3 days if trigger factor is controlled. Initiate oral fludrocortisone 0.1mg/day, or oral hydrocortisone preparation 30mg/day, when saline solution has been stopped.5.3 Prevention of acute adrenal insufficiency
Do not discontinue corticosteroids suddenly The dose must be doubled in patients with chronic adrenal insufficiency in the presence of stress Dexamethasone 4mg (TB) every 12 hours in cases of severe stress Pay attention to avoid dehydration, prevent infection, other factors. Predisposing factors Treat co-morbidities, if present Improve fitness, supplement with essential vitamins STTCs are common in the setting of undiagnosed or untreated underlying chronic adrenal insufficiency (Addison) full. It can also occur after a prolonged course of corticosteroid therapy, or as the result of many other pathological processes. Prompt treatment often saves the patient. Symptoms of the disease are similar to many other common serious illnesses. When left untreated, the disease progresses to shock unresponsive to fluids and vasopressors, causing death.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.
Customers can directly go to Vinmec Health system nationwide to visit or contact the hotline here for support.