
Cases requiring coronary angiography for emergency intervention
Posted by Doctor Nguyen Van Phong - Cardiology Center, Vinmec Times City International Hospital
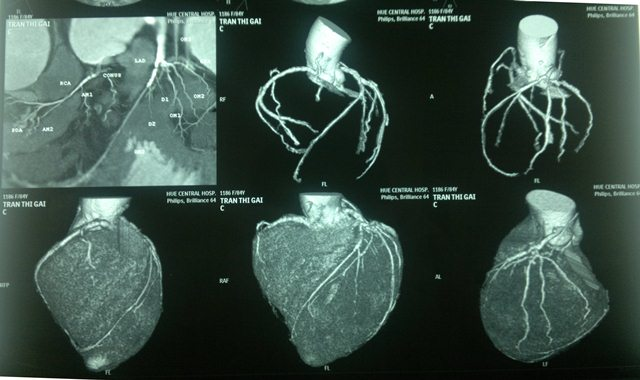
Emergency intervention coronary angiography is an invasive procedure that accurately diagnoses coronary artery stenosis, unclogs the blocked coronary artery, and improves blood flow to the heart.
1. Coronary angiography for emergency intervention
Coronary angiography considers emergency intervention as a necessary and preferred intervention when the patient is diagnosed with acute coronary syndrome. When this procedure is indicated, the patient should coordinate with the doctor's instructions. The best time from the time the patient was admitted to the emergency room until the patient was revascularized was within 90 minutes.
Acute coronary syndrome is an emergency of Cardiology related to coronary artery disease, which has the potential to affect the patient's life.
Symptoms, typical coronary artery-type chest pain: Aching (squeezing) strangulation behind the sternum, can spread to the left shoulder, to the chin, to both shoulders, the pain usually appears after an exertion but pain can occur even at rest, the pain usually lasts more than 20 minutes. Common clinical conditions: New onset angina, or increasing angina, angina occurring after events or procedures such as: after myocardial infarction, coronary intervention (CAD) ), coronary artery bypass graft surgery, many patients do not have clear pain symptoms but just a feeling of heavy pressure and difficulty breathing (silent pain).
2. Acute coronary syndrome
Non-ST-elevation acute coronary syndromes include two clinical presentations: non-ST-elevation MI (NSTEMI) and unstable angina. Clinically and electrocardiographically, there is no difference between these two conditions, the difference is that non-ST-elevation MI is increased myocardial biomarkers on laboratory tests and unstable angina. determined no. Immediately upon admission, the patient will be evaluated for chest pain, overall assessment of functional symptoms and comprehensive physical examination, identification of complications (if any): Cardiac arrhythmia, acute pulmonary edema , cardiogenic shock, ... to have a timely emergency attitude, conduct some investigations and tests right away to stratify the risk and devise an appropriate treatment strategy. Then, depending on the situation, how the patient accesses the health system (the center is capable of coronary intervention or not) to make the decision to transport the patient to the center that has the ability to intervene. .
Because the purpose of coronary angiography is to intervene if possible, coronary angiography in non-ST-elevation ACS is indicated in very high, high, or moderate risk patients. The duration of the scan depends on the level of risk stratification. If the patient is at very high risk (ie, the mortality and cardiovascular events are very high if not treated promptly), the patient will receive emergency coronary intervention in 2 hours. For patients with high or moderate risk, they will receive emergency coronary intervention within 24 hours. In general, in cases where an invasive approach is indicated, patients with non-ST-segment elevation acute coronary syndromes should be prioritized for percutaneous coronary angiography and acute coronary intervention if possible.
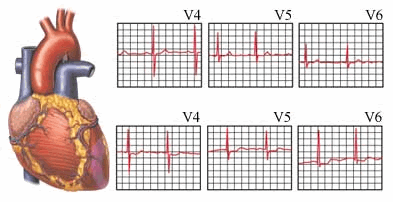
Acute coronary syndrome with ST-segment elevation is diagnosed when the criteria for acute MI are met and there is ST-segment elevation on the electrocardiogram. The diagnosis is usually established as soon as the electrocardiogram (ST segment elevation or new bundle branch block appears) at the patient's visit. This is different from the non-ST-segment elevation MI or unstable angina because the diagnostic process may be slower after identifying changes in myocardial biomarkers. All patients with suspected ST-segment elevation acute MI should be monitored continuously in the intensive care unit. Pre-established peripheral intravenous line, pain relief and optimal medical treatment. Coronary revascularization is mandatory and should be carried out as soon as possible and is the fundamental principle of the treatment of acute ST-segment elevation MI, a race against time, with the motto: “Time is the heart muscle, heart muscle is life”. Because experimental studies as well as clinical trials have shown the benefit of myocardial preservation when the coronary artery is recanalized early.
3. Coronary revascularization measures
Current coronary revascularization measures include the following main measures:
Use of thrombolytic drugs . Interventional coronary artery bypass catheter. Acute coronary artery bypass graft surgery is indicated when intervention is not possible or when there are complications. From 0 to 12 hours from the onset of symptoms, coronary intervention is the first choice.
From 12 - 48 hours from the onset of symptoms: It is mandatory to appoint coronary angiography and intervention in the first place if the patient has recurrent chest pain, arrhythmia or hemodynamic instability.
For other patients (stable, symptom-free patients) only initial coronary intervention should be considered. The first intervention should be selected at qualified and experienced facilities if the estimated time from first access to medical staff to coronary artery bypass grafting is ≤ 120 minutes (if moving to another place). ) or 90 minutes (if the patient arrives immediately to a health facility for acute intervention), ideally 60 minutes for acute MI that arrives 2 hours early or a large infarct area (eg. anterior MI).
In addition, in acute MI, patients should receive dual antiplatelet therapy including aspirin and a P2Y12 receptor antagonist (Ticagrelor or Prasugrel, or Clopidogrel if ticagrelor or prasugrel is not available or if these two drugs are contraindicated. ) for at least 12 months, unless there are major bleeding complications.
To protect cardiovascular health in general and detect early signs of coronary heart disease, customers can sign up for the Cardiovascular Screening Package of Vinmec International General Hospital. The examination package helps to detect cardiovascular problems at the earliest through tests and modern imaging methods. The package is for all ages, genders and is especially essential for people with risk factors for cardiovascular disease.
Why should you choose Cardiovascular Screening Package at Vinmec International General Hospital?
Simple and quick procedure. Enthusiastic advice and support, reasonable and convenient examination process. Comprehensive facilities, including a system of clinics and consultations, blood collection rooms, dining rooms, waiting areas for customers,... Highly qualified medical staff, Professional working style, dedicated and attentive.
Để đặt lịch khám tại viện, Quý khách vui lòng bấm số HOTLINE hoặc đặt lịch trực tiếp TẠI ĐÂY. Tải và đặt lịch khám tự động trên ứng dụng MyVinmec để quản lý, theo dõi lịch và đặt hẹn mọi lúc mọi nơi ngay trên ứng dụng.
Dịch vụ từ Vinmec
-
 Công dụng thuốc Abciximab
Công dụng thuốc AbciximabThuốc Abciximab được bào chế dưới dạng thuốc tiêm tĩnh mạch, có thành phần chính là Abciximab. Thuốc được sử dụng để ức chế kết tập tiểu cầu, chống huyết khối. Để đảm bảo hiệu quả điều trị và tránh ...
Đọc thêm -
 Hồi hộp (đánh trống ngực) : dấu hiệu của bệnh gì?
Hồi hộp (đánh trống ngực) : dấu hiệu của bệnh gì?Hồi hộp (đánh trống ngực) là tình trạng người bệnh cảm nhận được nhịp tim của mình đang đập trong lồng ngực, cảm nhận nhịp tim nhanh, mạnh hoặc không đều và thường được bệnh nhân mô tả là tim ...
Đọc thêm -
 Phương pháp siêu âm IVUS có đánh giá được nguy cơ hẹp mạch vành không?
Phương pháp siêu âm IVUS có đánh giá được nguy cơ hẹp mạch vành không?Người nhà em năm nay đã 81 tuổi, đau ngực và đi chụp mạch vành thì phát hiện ra bị hẹp trên 1 đoạn rất dài mạch vành, có vị trí hẹp tới 95%. Vậy bác sĩ cho em hỏi ...
Đọc thêm -
 Công dụng thuốc Eptifibatide
Công dụng thuốc EptifibatideEptifibatide chứa thành phần chính là Eptifibatide với hàm lượng 0,75mg/1ml - một chất ức chế kết tập tiểu cầu, thuộc phân nhóm giống RGD (Arginine Glycine - Aspartate). Thuốc được sử dụng để điều trị cho bệnh nhân mắc ...
Đọc thêm -
 Can thiệp mạch vành qua da và ghép bắc cầu động mạch vành khác nhau ra sao?
Can thiệp mạch vành qua da và ghép bắc cầu động mạch vành khác nhau ra sao?Bệnh động mạch vành, hay CAD, là một bệnh tim thường được điều trị thông qua việc sử dụng thuốc, thay đổi lối sống cùng chế độ ăn uống. Trong trường hợp tình trạng trở nên nghiêm trọng, bác sĩ ...
Đọc thêm