This is an automatically translated article.
The article was consulted with Master, Doctor Tran Mai Phuong - Pediatrician - Department of Pediatrics - Neonatology, Vinmec Central Park International General Hospital.Atypical pneumonia is a lung infection caused by atypical bacteria. Children with atypical pneumonia often have milder symptoms than typical pneumonia, even difficult for parents to realize that the child is sick.
1. Overview of atypical pneumonia
The term atypical pneumonia first appeared in 1938 and tends to increase day by day. The prevalence of atypical pneumonia accounts for about 15-25% of all pneumonia cases in general.This is a bacterial infection that can be contracted by anyone of any age. However, the most common subjects are children aged 2-10 years old or adults under 40 years old, of which pre-school age accounts for 75-80%.
People who live and work in crowded places, such as schools, homeless shelters or prisons, are often at higher risk of illness. Infection occurs when a person comes into contact with an infected person's saliva or nasal secretions when coughing or sneezing.
It is important when treating atypical pneumonia in children that a full course of antibiotics is given. If antibiotics are stopped too soon, the risk of re-infection is very high. If not treated promptly, atypical pneumonia also has the risk of leading to dangerous complications.

Viêm phổi không điển hình ở trẻ em
2. Causes of atypical pneumonia
There are 3 types of bacteria that cause atypical pneumonia:Mycoplasma pneumoniae: accounting for 55 - 70% of cases, mainly affecting people under 40 years old; Chlamydia pneumoniae: Accounts for 10-15% of cases, most common in school-age children and usually shows only mild symptoms; Legionella pneumoniae: accounts for 5 - 7% of cases, but can be more severe than other forms. The most common form of atypical pneumonia is caused by the bacteria Mycoplasma. The proportion of healthy people carrying atypical bacteria in the community accounts for about 30-35%.
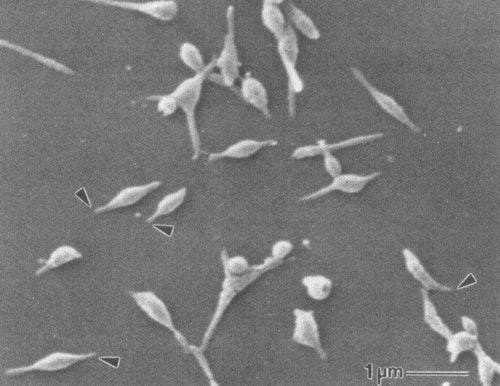
Hình ảnh vi khuẩn Mycoplasma pneumoniae
3. Clinical symptoms of atypical pneumonia
Most cases of atypical pneumonia begin with respiratory symptoms, sometimes with a sudden rapid onset. In addition, children with atypical pneumonia also have the following suggestive clinical features:Usually high fever > 39 - 40°C and continuous. For infants, young children or the elderly can also have pneumonia without fever , even hypothermia; Cough with multiple episodes or dry cough initially, later with sputum; Hoarseness due to coughing a lot; Older children may have chest pain; Physical symptoms (feeling by the child) are often overwhelming; Physical symptoms (clinical manifestations) are often poor, less obvious; Faster breathing rate for age; Older children may not have rales, while young children may have moist and bronchial rales, but they appear quite late; Often combined with extrapulmonary lesions such as: pleura, liver, spleen or myocardium...

Trẻ liên tục sốt cao
4. Diagnosis of atypical pneumonia
In order to make a definitive diagnosis, in addition to considering the age of the pediatric patient, epidemiological factors and clinical manifestations, the doctor will also rely on laboratory tests that are valuable to suggest atypical pneumonia as follows:4.1. Hematology tests Blood counts in a CBC in children with atypical pneumonia show:
Normal or slightly increased white blood cell count; The percentage of neutrophils may not be increased; C-reactive protein (CRP) is usually normal. 4.2. Biochemical tests Little change; 4.3. Microbiological test Microbiological test helps to analyze microbial images, has diagnostic value to determine the cause of disease bacteria. For atypical pneumonia in children, doctors can find evidence of atypical bacterial DNA fragments from respiratory secretions by:
Direct bacterial culture method; PCR molecular biology test: Mycoplasma pneumoniae / Chlamydia pneumoniae / Legionella pneumoniae nasopharyngeal, endotracheal or pleural (+); Real time series fusion (Real time PCR technique).

Xét nghiệm máu chẩn đoán viêm phổi không điển hình
Mainly parenchymal lesions, diffuse, reticular, irregularly blurred, scattered in the entire 2 lung fields of the type of interstitial pneumonia; Sometimes there is concentrated pneumonia, dark opacities, necrotic-type focus; Some cases have pleural effusion on 1 or 2 sides but the volume of fluid is not much. Doctors need to do a physical examination and perform laboratory tests to diagnose pneumonia. In which, symptoms such as fever, cough, rapid breathing, chest indrawing are the most important for clinical diagnosis and determining the severity of the disease. The paraclinical tests are ordered by the doctor after the parents bring a child with suspected pneumonia to visit
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of professional staff. leading medical doctors, modern technology equipment system. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
5. Treatment of atypical pneumonia
5.1. Anti-respiratory failure In the case of atypical pneumonia in children with respiratory failure, it is necessary to:Use oxygen therapy; Closely monitor breathing rate, SaO2, blood gases and clear airways; Administer fluids to provide adequate fluids and electrolytes to the pediatric patient. 5.2. Supportive treatment The principle of supportive treatment includes reducing fever and providing adequate nutrition and calories according to the child's needs.
5.3. Antibiotic therapy For atypical pneumonia, the first choice is the macrolide antibiotic Azithromycin at 10 mg/kg on day 1, followed by 5 mg/kg/day once daily for 2 - 7 days.
Oral alternatives for 10-14 days include:
Clarithromycin: 15 mg/kg/day in 2 divided doses; Erythromycin: 40 - 50 mg/kg/day divided into 4 times; Doxycycline: 2 - 4 mg/kg/day in 2 divided doses for children > 7 years old. If the child is allergic to Macrolid, the next group of antibiotics should be replaced, which is also highly effective against bacteria that cause atypical pneumonia, which is Quinolone. Specifically:
Levofloxacin: 20 mg/kg/day for children < 5 years old or 10 mg/kg/day for children > 5 years old or 500 mg once daily for children > 15 years old; Or moxifloxacin: 400 mg once daily for children over 15 years of age. Use oral form with non-severe pneumonia (without respiratory failure). If the child has atypical pneumonia with respiratory failure, the antibiotic Azithromycin or Lactobionate erythromycin / levofloxacin should be given intravenously.
The duration of antibiotic therapy usually lasts from 5-14 days. For children with immunodeficiency, severe illness and pneumonia caused by L.pneumophila, treatment will last about 14-21 days.

Gia đình nên đưa trẻ đến gặp bác sĩ để được thăm khám và điều trị kịp thời
6. Follow-up treatment and treatment
During treatment, there is a possibility of co-infection, drug resistance or extrapulmonary complications causing treatment failure with the following signs:Fever lasting more than 48 hours; Increased respiratory failure; Increased parenchymal lesions on 2 lobes of the lung; Extrapulmonary manifestations are present. At that time, the doctor may conduct a number of tests over time and depending on the course of the disease as well as extrapulmonary manifestations, such as blood cultures, endotracheal intubation, chest CT, pleural ultrasound, electrolytes , ...
If resistance occurs, consider changing Macrolide antibiotics to Quinolones, or using antibiotics according to the antibiogram in case of co-infection. In pediatric patients with severe pneumonia caused by M.pneumoniae, corticosteroids may be considered.
However, in general, cases of atypical pneumonia are fully reversible with a full course of antibiotic therapy. Currently, there is no specific vaccine to prevent atypical pneumonia in children caused by this group of 3 bacteria. Parents can prevent their children from getting pneumonia mainly by getting enough nutrition, getting their immunizations on schedule, and limiting the impact of a polluted environment.
As a key area of Vinmec Health system, Pediatrics Department always brings satisfaction to customers and is highly appreciated by industry experts with:
Gathering a team of top doctors and nurses in Pediatrics : consists of leading experts with high professional qualifications (professors, associate professors, doctorates, masters), experienced, worked at major hospitals such as Bach Mai, 108.. Doctors All doctors are well-trained, professional, conscientious, knowledgeable about young psychology. In addition to domestic pediatric specialists, the Department of Pediatrics also has the participation of foreign experts (Japan, Singapore, Australia, USA) who are always pioneers in applying the latest and most effective treatment regimens. . Comprehensive services: In the field of Pediatrics, Vinmec provides a chain of continuous medical examination and treatment services from Newborn to Pediatric and Vaccines,... according to international standards to help parents take care of their health. From birth to adulthood Specialized techniques: Vinmec has successfully deployed many specialized techniques to make the treatment of difficult diseases in Pediatrics more effective: neurosurgery - skull surgery, cell transplantation. hematopoietic stem in cancer treatment. Professional care: In addition to understanding children's psychology, Vinmec also pays special attention to the children's play space, helping them to have fun and get used to the hospital's environment, cooperate in treatment, improve the efficiency of medical treatment.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.