This is an automatically translated article.
The article was professionally consulted by MSc, Dr. Trinh Thi Thanh Huyen - Obstetrician and Gynecologist - Department of Obstetrics and Gynecology - Vinmec Hai Phong International General HospitalPostpartum obstetrical bleeding is a major life-threatening risk. This is an obstetric emergency, the patient needs resuscitation and active intervention. Partial hysterectomy and ligation of the hypogastric artery may be an option if medical therapy is ineffective.
1. Indications for partial hysterectomy and hypogastric artery ligation
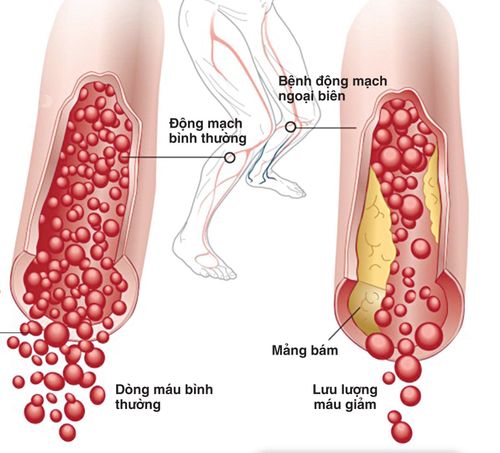
Postpartum obstetric bleeding is one of the most dangerous obstetric complications. Postpartum obstetric bleeding is defined as the loss of more than 500 ml of blood during and immediately after vaginal delivery or cesarean section. .
When postpartum obstetric bleeding occurs, the patient will be actively resuscitated, set up a line, and contract the uterus with drugs such as Oxytocin, Methyl-ergometrin, Carbetocin, ... in combination with uterine fundus. , check the vagina and cervix, use prophylactic antibiotics. If the above measures are not effective, we will switch to performing surgical interventions.
Partial hysterectomy and ligation of the hypogastric artery is one of the obstetric surgeries that can be indicated in cases of bleeding secondary to cesarean section.

Cắt tử cung bán phần giúp điều trị chảy máu sản khoa sau sinh
2. What is the process of partial hysterectomy and hypogastric artery ligation?
2.1 Preparation process
Experienced obstetrician and surgical assistant team. Equipment: Gynecological surgery kit, sterile surgical instruments, cotton, gauze, needles, good quality thread, Neslaton catheter, Disteur used to dissect and expose hypogastric and urinary arteries manage . Patient: Prepare patient as an obstetric emergency, perform necessary tests, recheck blood parameters to assess blood loss, advise patient on surgical goals and complications may occur, carefully examine the perineum and anal sphincter to detect lesions if vaginal delivery.
2.2 Steps to take
Stage 1: Open the abdomen according to the incision of the previous cesarean section, the transverse line above the pubic joint or the midline below the navel. Then 2: Carry out clamping to cut the round ligament. Stage 3: Perform peritoneal dissection of the lower part of the uterus, pushing down, separating the bladder from the uterus. Stage 4: If the appendage is removed, the ovary lumbar ligament is cut, if the appendage is left, the fallopian tube-ovarian ligament is cut. Stage 5: Perform bilateral uterine artery ablation at the level or slightly below the part of the uterus to be removed, the location of the cutting pair is usually across the border between the body of the uterus and the cervix. Stage 6: Carry out a hysterectomy, usually cut in a wedge shape for easy hemostasis, and the cervix is left. Stage 7: Suture the cutting apex, cover the cut peritoneum. Then 8: If indicated, perform hypogastric artery ligation. Ligation of the hypogastric artery is performed according to the following steps: Incision of the posterior peritoneum corresponding to the position of the hypogastric artery. Determine the landmark at the position of 2-3cm to the right and left of the protrusion. Use forceps to pull up the peritoneal fold to cut a hole in the posterior peritoneum at the right spot. Then, with blunt curved scissors, separate the peritoneum and cut the peritoneum about 4 cm downward along the path of the internal iliac artery. Expose the ureter and hypogastric artery by closed curvilinear traction. Hypogastric artery ligation: Using obtuse curvilinear forceps, threaded through the inferior surface of the hypogastric artery and anterior to the hypogastric vein from the outside to the inside. When the clamp is clearly visible at the medial border of the hypogastric artery, open the clamp at the clamp and thread the thread through the hypogastric artery. When determining that the thread has been threaded in the correct position under the hypogastric artery, perform a ligation of the hypogastric artery, cutting the suture 1cm away from the knot. Stage 9: Check for bleeding and ureters on both sides. Stage 10: Proceed to close the abdominal wall according to anatomical layers.
3. Complications may occur after partial hysterectomy and hypogastric artery ligation

Bệnh nhân có thể gặp phải tai biến chảy máu và rối loạn đông máu khi phẫu thuật
The most common complications are bleeding and coagulation disorders. Bleeding occurs when the surgeon does not tie the vessels properly, the cause of clotting disorders is prolonged bleeding. In order to prevent the above case, during surgery, the surgeon needs to tie the vascular peduncles firmly, depending on the patient's blood loss, blood transfusion and clotting agents are indicated. After surgery, the patient should be closely monitored for pulse, blood pressure and hemodynamic indicators. Insert an abdominal tube if there is a coagulopathy.
Postpartum obstetric bleeding is an unpredictable risk, all pregnant women are considered at risk because more than 40% of postpartum bleeding cases have no known cause. Partial hysterectomy and hypogastric artery ligation are highly effective surgical procedures in the treatment of bleeding after cesarean section. However, this is a difficult technique, the success of the operation depends greatly on the skill of the doctor and the physical conditions and equipment for the surgery.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
Reference source: Manual of the Ministry of Health