This is an automatically translated article.
Posted by Master, Doctor Ha Thi Thu Hien - Pathologist - Laboratory Department - Vinmec Times City International HospitalPapillary carcinoma is a common form of thyroid cancer that is caused by exposure to radiation energy. The disease usually presents as irregular nodules or cysts or tumors in the normal thyroid parenchyma. Once advanced, papillary carcinoma of the thyroid gland can be minimally or excessively invasive.
1. What is papillary carcinoma of the thyroid gland?
Papillary carcinoma is a malignant tumor differentiated from thyroid follicular epithelial cells, typically having a papillary or follicular structure with distinct nuclear features. There are many variations of the different papillary structure, but the nuclear characteristics remain unchanged (large nucleus, translucent glass, pale, grooved, intranuclear inclusions).
2. Epidemiology Papillary carcinoma of the thyroid gland is the most common malignancy of the thyroid gland, accounting for 80% of thyroid malignancies.
The number of thyroid papillary carcinomas has been increasing in the last 15 - 20 years due to an increase in the detection of very small nodules in the thyroid on ultrasound, computed tomography but most of these tumors low risk.
Thyroid papillary carcinoma occurs in all ages, including children and young adults, but is most common in the 20-74 age group. Female predominance with an F:M ratio of 3:1
3. Causes of papillary adenocarcinoma Although the etiology of thyroid papillary carcinoma is unknown, several factors are involved. The effects are recognized as: the impact from the radiation of the living environment. In addition, many other risk factors have also been identified, including reproductive factors, obesity, diabetes, smoking, alcohol consumption, excess iodine in the diet... and other factors. genetic. However, the relationship between these factors and thyroid papillary carcinoma is not entirely clear.

Người béo phì thuộc nhóm nguy cơ cao mắc bệnh ung thư biểu mô tuyến nhú
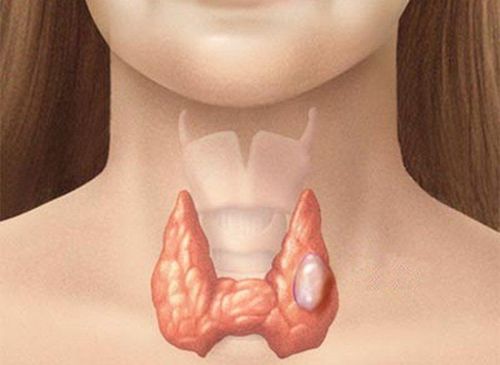
4. Clinical Manifestations of Papillary Carcinoma The clinical presentation of papillary carcinoma is often indistinct. The main symptom is a painless mass in the thyroid gland, enlarged or non-enlarged cervical lymph nodes. In fact, any part of the thyroid gland can become a tumor.
Risk of thyroid papillary carcinoma in patients with goiter. Previous studies comparing patients with multinodular goiter with those with one thyroid nodule showed no difference in cancer incidence. Later studies suggested that patients with isolated thyroid nodules had a higher risk of thyroid papillary carcinoma than patients with multiple thyroid nodules. However, these views are no longer true as many subsequent studies have reported a significant risk of thyroid papillary carcinoma in patients with multiple thyroid nodules. Therefore, thyroid papillary carcinoma is the most common thyroid malignancy discovered incidentally in patients with benign goiter. The risk of thyroid papillary cancer in multinodular goiter has been reported to vary from as low as 6% to as high as 21.2%.
5. Diagnosis of papillary carcinoma of the thyroid gland
5.1. Thyroid cytology aspiration Thyroid cytology is the method of choice for the diagnosis of papillary thyroid carcinoma. This is a minimally invasive and rapid procedure, they are performed by using a fine needle to take a sample of the lesion, spread it on a slide and analyze it under the microscope with the following common features:
Plate many cells, little or no colloid. Characteristic characteristics that determine the diagnosis of TPC include: Large, abnormal in shape and size; Chromatin granular, powder; Pseudo-implantation in the nucleus; Kernel has knurled; Multiply, superimposed. The cytoplasm is broad, pale, hollow, and foamy. Cytoplasmic features are not helpful in diagnosis. Sand bodies may be present, which is of great help in diagnosis.
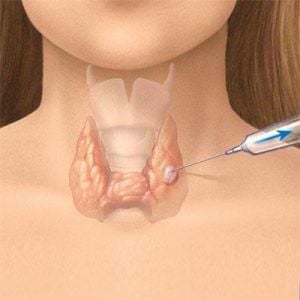
Kỹ thuật chọc hút tế bào tuyến giáp được áp dụng trong chẩn đoán ung thư biểu mô nhú tuyến giáp
To increase the diagnostic accuracy of thyroid cytology, ultrasonography is a valuable technique in selecting suitable suspected nodules for cytology in a multinodular thyroid gland. It can detect very small lesions that the doctor may not be able to detect on physical examination. In addition, ultrasound also provides the exact size of a nodule to monitor for the patient.
5.2 Cryosection or immediate intraoperative biopsy (Frozen section) Cryosection is strongly discouraged because the effect of freezing distorts nuclear features essential for diagnosis.
Preoperative fine needle aspiration cytology to confirm the diagnosis and determine the most appropriate surgical procedure.
Cryosection in thyroid surgery is often used to detect tumor invasion into parathyroid tissue and sometimes lymph node metastasis.
5.3. Macroscopic picture Most TPCs are solid masses, with unclear boundaries, invading the thyroid parenchyma or surrounding tissue. May be solid, cystic or simply cystic. The type of cyst usually has a shell, the interior is bright or contains a yellow-brown fluid, papillae can be seen in the cyst wall. Fibrosis is common in and around the tumor. May be fairly homogeneous granules, may have multiple foci of calcification or ossification. 5.4 Microscopic image Structural features:
Growth form: papillary, cystic, solid, raft, organization. There can be more than one type on one u. The cyst is elongated, twisted, and less colloidal. Sand body. Abnormal fibrosis in the tumor. The glue is denser than the surrounding thyroid tissue. Has a papillary structure that protrudes into the lumen of the cyst. Scaly metaplasia (50%).
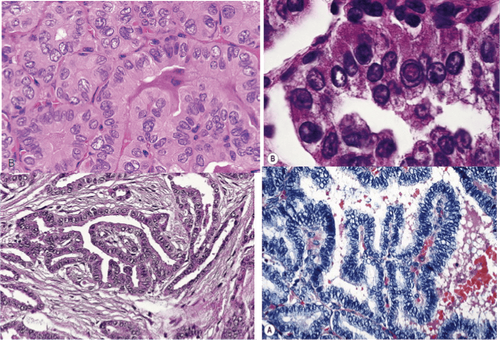
Hình ảnh carcinôm tuyến giáp dạng nhú (vi thể)
Cell characteristics (nuclear characteristics):
Large nucleus. Unusual multiplication in shape and size. Chromatin dispersion or creation of the nucleus image “Orphan Annie”. Chromatin is concentrated along the nuclear membrane. The nucleus is no longer located along the basement membrane but is arranged randomly within the cell. Multiply up and down (crowding), multiply on top of each other (overlapping). Pseudohyperophilic inclusions in the nucleus. The kernel has notches and grooves. If a nucleus is present, it is usually located along the nuclear membrane. Cytoplasmic features have no diagnostic value. 6. Prognosis and treatment of papillary carcinoma poor prognostic factors of thyroid papillary carcinoma include old age at the time of diagnosis, sex, large tumor size,...
Surgery Surgery is often the first-line therapy for papillary carcinoma of the thyroid gland. The extent of surgery depends on the size of the primary tumor and the presence of lymph node metastases. Iodine or tyrosine kinase inhibitors can be used depending on the case.
Previously, the recurrence of papillary thyroid cancer was quite low, the survival rate was 99% after 20 years of surgery. However, in some studies it has been reported that more than 25% of patients have been found to have recurrent thyroid papillary carcinoma during a long follow-up period. In which, 11% of cases recur after 20 years of treatment, so doctors often recommend that patients with a history of papillary thyroid carcinoma need to be monitored and periodically re-examined.

Một số trường hợp, người bệnh được điều trị nội khoa bằng thuốc ức chế tyrosine kinase
Currently, Vinmec International General Hospital has a package of screening and screening for thyroid diseases. When choosing the Package of Screening and Screening for Thyroid Diseases at Vinmec, you will be examined by experienced thyroid specialists to help screen and detect common thyroid diseases early. variables such as: simple goiter, hyperthyroidism, hypothyroidism, thyroiditis, thyroid nodules, thyroid cancer,...
At the same time, you will have blood tests, evaluate the levels of functional hormones. thyroid such as FT3, FT4, TSH, Anti - TPO, Anti TG and ultrasound, scan to evaluate the structure of the thyroid gland. After that, when the results are returned to the doctor, you will be consulted about thyroid pathology, and discuss the appropriate treatment options for yourself. From there, thyroid disease will be prevented in time, avoiding long-term health damage in the future.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
SEE ALSO:
Papillary thyroid tumor: Pathological progression and diagnostic methods Does benign thyroid tumor require surgery? TSH hormone and its significance in the screening diagnosis of thyroid diseases