This is an automatically translated article.
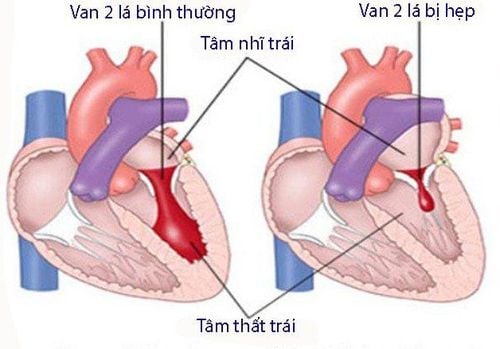
The article was written by a doctor at the Heart Center, Vinmec Times City International General HospitalThere are many causes that can lead to mitral regurgitation: rheumatic heart disease, degeneration, rupture of valvular ligaments, infective endocarditis, coronary artery disease, cardiomyopathy... About 2% of the population has this disease. .
1. How it manifests Most people with mitral regurgitation have no symptoms. People with mild or moderate mitral regurgitation may never have symptoms or complications. Even patients with severe mitral regurgitation in the early stages are asymptomatic until left ventricular failure, arrhythmias, or pulmonary hypertension. Patients will have manifestations of heart failure with the following symptoms: Fatigue, shortness of breath on exertion and later appearing even at rest, edema of the lower extremities.

Hầu hết những người hở van hai lá không có triệu chứng
2. Diagnosis The doctor will perform a physical examination to guide the diagnosis. Auscultation will detect a systolic murmur caused by reflux from the left ventricle to the left atrium. Other investigations include:
Cardiopulmonary x-ray: detects enlarged heart and pulmonary edema.
Electrocardiogram : to detect associated arrhythmias. The electrocardiogram also shows the effect of mitral regurgitation on the whole heart structure, stenotic coronary lesions if present.
All patients with suspected mitral regurgitation are indicated for echocardiography to confirm the diagnosis and determine the degree of regurgitation. Echocardiography can also diagnose the cause of the disease. In patients with severe mitral regurgitation but no symptoms or obvious symptoms, echocardiography every 6 months can be used to assess the degree of left ventricular dilatation as well as changes in ventricular contractile function. left. Then determine the right time for surgery. Stress echocardiography can also be used to determine the degree of valvular regurgitation, pulmonary artery pressure, and exercise left ventricular reserve in asymptomatic patients. In cases where transthoracic ultrasound does not give a clear image, transesophageal ultrasound can be used to observe the mitral valve closer for more accurate results.
In some cases where mitral regurgitation is suspected as a consequence of coronary artery disease or comorbid coronary artery disease, catheter angiography is required.
3. Patient's progress Patients with mild mitral regurgitation do not need to be monitored and examined periodically. People with moderate and many clefts need to be monitored and examined periodically for timely treatment. The frequency of visits will be according to the doctor's advice based on the degree of valve regurgitation, the degree of dilatation of the heart, and the severity of symptoms. In general, when symptoms are present or symptoms increase, it is necessary to see a doctor at least every 6 months.
If the patient is asymptomatic, has a regular rhythm, and normal left ventricular and left atrial size, and normal pulmonary artery pressure, there may be no need to limit physical activity.

Effects of childbirth for patients with mitral regurgitation: Usually, patients with mitral regurgitation adapt quite well to childbirth, especially those with minor regurgitation and no symptoms or very mild symptoms. But conversely, if there are already symptoms or complications, there is a high chance that serious complications will appear at birth. If you are in the latter group of patients and you need to have a baby, it is best to see a cardiologist who is counseled about the risks of childbirth and the possibility of an anterior mitral valve repair or replacement surgery. Mitral valve surgery is not recommended during pregnancy, except in emergencies.
Atrial fibrillation in mitral regurgitation: is an electrical disturbance in the atria manifested by rapid and irregular atrial rhythms. In patients with mitral regurgitation, the normal amount of blood pumped by the heart has decreased, atrial fibrillation further reduces this blood volume and significantly increases the risk of stroke, or limb embolism due to the formation of blood clots in the chambers. heart. Patients with atrial fibrillation are treated with anticoagulants and may receive medication (or electric shock) to return the rhythm to normal. Patients with atrial fibrillation are recommended to undergo early surgery when the left atrium is not dilated much, affecting the ability to convert during surgery.
4. How to treat The decision to treat depends on the degree of valve regurgitation, the patient's symptoms as well as the cause of the mitral regurgitation. Most patients with severe mitral regurgitation will require surgical repair or replacement of the mitral valve. In some cases surgery may be delayed if the patient has comorbidities.

Mitral valve repair surgery: Repairing and restoring closed mitral valve function will preserve myocardial function and avoid the patient having to take anticoagulants permanently. Mitral valve repair surgery is often more complicated than mitral valve replacement, so it requires a surgeon experienced in this technique.
Mitral valve replacement surgery : When the valve damage is severe, especially when due to rheumatic heart disease or the consequences of coronary artery stenosis, many cases require mitral valve replacement. There are two types of artificial valves used: mechanical valves (made from metal) and biological valves (made from biological products such as pig heart or bovine pericardium). Mechanical valves have the disadvantage of requiring lifelong vitamin K anticoagulants. Biological valves will fail over time, especially in patients under 65 years of age. In general, mechanical valves are used in patients younger than 65 years of age or with atrial fibrillation (anticoagulation is required). Biological valves are intended for use in patients over 65 years of age. Biological valves can be used in patients under 65 years of age with a normal heart rate. However, it is important to explain to the patient the benefit between the use of vitamin K antagonist anticoagulants and the risk of future valve replacement.
Maze surgery: When a patient has atrial fibrillation, the surgeon can perform additional Maze surgery by making additional cuts in the atria using radiofrequency, ultrasound, or cryotherapy to prevent these complications. Pathological current is the cause of atrial fibrillation. The surgeon will discuss with the patient and family the decision whether to perform Maze surgery or not because this surgery will prolong the surgery time and increase the risk of some complications.
Drug treatment: Treatment drugs work to reduce symptoms of heart failure, reduce the burden on the heart and avoid complications such as blood clots in the heart or mitral valve infection.
Vasodilators (eg ACE inhibitors) improve blood flow and reduce left ventricular burden. However, the effectiveness of this drug has not been proven in the long-term treatment of patients with mitral regurgitation.
Vitamin K antagonists are indicated for patients with atrial fibrillation or after mechanical mitral valve replacement.
Most patients with mitral regurgitation do not require antibiotics prior to oral and upper respiratory procedures. However, patients who have had mitral valve replacement should strictly follow the instructions for the use of prophylactic antibiotics before surgical procedures.
Currently, most cases will be indicated surgery to repair the mitral valve through the Mitraclip catheter. This is a very modern cardiovascular intervention technique. Vinmec Hospital is one of the few hospitals that implement this technique with a success rate of up to 95%, equivalent to the general rate in the world. In addition, Vinmec's Cardiology Department has always received much praise and satisfaction from domestic and international customers, being pioneers in successfully applying the world's most advanced techniques in the treatment of diseases. Heart.
A team of highly qualified and experienced specialists: qualified doctors from Master's to Professor's and Doctor's degrees, reputable in medical treatment, surgery, interventional cardiac catheterization. Intensive training at home & abroad. In particular, Prof. TS.BS Vo Thanh Nhan - Cardiology Director of Vinmec Central Park was recognized as the first and only expert in Vietnam to be awarded the "Proctor" certificate on TAVI. State-of-the-art equipment, comparable to major hospitals in the world: The most modern operating room in the world; The most modern silent magnetic resonance imaging machine in Southeast Asia; The CT machine has a super-fast scanning speed of only 0.275s/round without the use of drugs to lower the heart rate; 16-sequence PET/CT and SPECT/CT systems help to detect early damage to cardiovascular organs even when there are no symptoms of the disease. Applying the most advanced advanced cardiovascular techniques in the world in treatment: Painless open heart surgery; Percutaneous aortic intervention without general anesthesia; Treatment of mitral regurgitation through the catheter has a success rate of 95%; Ventricular-assisted artificial heart transplantation for patients with end-stage heart failure prolongs quality of life beyond 7 years. Cooperating with leading cardiovascular centers in Vietnam and the world such as: National Heart Institute, Cardiology Department of Hanoi Medical University, University of Paris Descartes - Georges Pompidou Hospital (France), University of Pennsylvania (France), University of Pennsylvania United States)... with the aim of updating the most modern cardiovascular treatments in the world. To be examined by leading Cardiologists, please register online at the website or contact Vinmec Health System nationwide.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.