This is an automatically translated article.
The article was professionally consulted with Master, Doctor Doan Ngoc Quynh - Pediatrician - Pediatric Center - Vinmec Times City International Hospital.The process of cervical cancer often begins with precancerous changes, and there are ways to stop the disease from developing. The first way is to find and treat pre-cancers before they become actual cancers, and the second way is to prevent pre-cancers.
1. HPV vaccine still effective when infected with HPV virus?
The HPV vaccine can protect young people against some infections caused by HPV. These vaccines help prevent pre-cancer and cervical cancer. Some HPV vaccines are also approved to help prevent other types of cancer, anal and genital warts.These vaccines only work to prevent HPV infection - they will not work against an already existing infection. That's why, to be most effective, the HPV vaccine is recommended before a person is exposed to the virus (such as through sexual activity). In case of infection, it is still possible to inject because this is an active antibody. However, you should consult your doctor for follow-up after injection.
The vaccine requires a series of shots. Side effects are usually mild. The most common is short-term redness, swelling, and soreness at the injection site.
The American Cancer Society's recommendations for the use of the HPV vaccine are similar to those from the Federal Advisory Committee on Immunization Practices (ACIP), and include:
Should be started. routine HPV vaccine for girls and boys at age 11 or 12. Vaccination can be started as early as age 9.
HPV vaccination is also recommended for 13- to 26-year-old females and 13- to 21-year-old males who have not started vaccination or have started but not completed booster shots. Men between the ages of 22 and 26 can also be vaccinated.
HPV vaccination is also recommended until age 26 for men who have sex with men and people with weakened immune systems (including people with HIV), if they have not been vaccinated before.
For those 22 to 26 years of age who have not started a vaccine or have started but have not completed booster shots, it is important to know that the later the vaccine is given, the more effective it is at reducing cancer risk. mail will be less.
It is important to realize that no vaccine provides complete protection against all cancer-causing viruses, so routine cervical cancer screening remains important. necessary.

Vacxin HPV còn có tác dụng khi đã nhiễm virus HPV?
2. Treatment methods after cervical cancer is detected
2.1 Stage 0 (carcinoma in situ) Although the AJCC staging system classifies carcinoma in situ (CIS) as the earliest form of cervical cancer, doctors often think of it as precancerous. That's because the cancer cells in the CIS are only in the surface layer of the cervix, they don't grow into the deeper layers of cells.All cases of CIS can be cured with the right treatment. However, precancerous changes can sometimes recur in the cervix or vagina, so patients still need to be closely monitored after treatment. This includes follow-up with routine Pap tests and in some cases colposcopy.
Treatment options for squamous cell carcinoma in situ include:
Cryosurgery Laser surgery Electron loop ablation procedure (LEEP/LEETZ) Cold knife Simple hysterectomy (is first-line treatment or if cancer comes back after other treatments) Treatment options for adenocarcinoma in situ include:
Hysterectomy Conical biopsy (a viable option for women who want to have children). The cone specimen must be free of cancerous cells at the margins and the woman must be closely monitored after treatment. Once a woman has given birth, the uterus should be removed. 2.2 Stage IA1 Treatment for this stage depends on whether you want to continue having children (maintain fertility) and whether the cancer has entered the bloodstream or lymphatic vessels (called lymph node invasion). blood).
Treatment options for women who want to maintain fertility:
A cone biopsy is the preferred procedure for women who want to have children after cancer treatment. If the edges of the cone contain cancer cells, the woman can be watched closely without further treatment as long as the cancer does not come back. If the edges of the cone biopsy have cancer cells, the cancer may have been left behind. This can be treated with repeat cone biopsies or radical mastectomy (removal of the cervix and upper vagina). This method is preferred if the cancer has spread to the blood or lymphatic vessels. Treatment options for women who do not wish to maintain fertility:
A total hysterectomy may be an option if the cancer shows no lymph node involvement. If cancer has grown into the bloodstream or lymph nodes, a radical hysterectomy along with removal of the pelvic lymph nodes is needed.
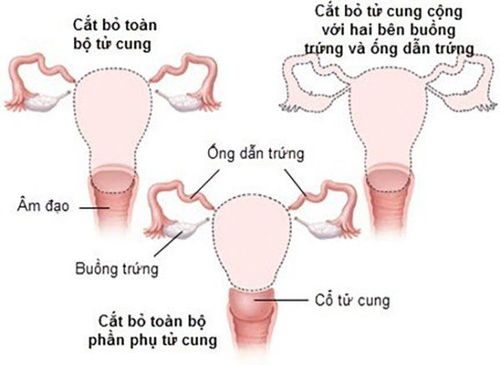
Phẫu thuật cắt toàn bộ tử cung có thể là một lựa chọn nếu ung thư cho thấy không có sự xâm lấn hạch bạch huyết
Treatment options for women who want to maintain fertility:
Conical biopsy with removal of pelvic lymph nodes (pelvic lymph node dissection) Radical hysterectomy with pelvic lymph node dissection Treatment options for women who do not wish to maintain fertility:
External beam radiation therapy (EBRT) to the pelvis plus radiotherapy treatment Radical hysterectomy with removal of the uterus pelvic lymph nodes and aortic lymph node sampling If none of the lymph nodes are cancerous, radiation may still be discussed as an option if the tumor is large or the tumor has grown in blood or lymph, or the tumor invades the surrounding connective tissue that supports organs such as the uterus, bladder, or vagina (stroma). If the cancer has spread to tissues next to the uterus or to any lymph nodes, radiation therapy (EBRT) is usually recommended. Your doctor may also advise other methods of treatment after a combination of chemotherapy and radiation. 2.4 Stages IB1 and IIA1 Treatment options for women who wish to maintain fertility:
Radical hysterectomy with pelvic lymph node dissection Treatment options for women who do not wish to maintain fertility:
Radical hysterectomy by removing lymph nodes in the pelvis and some lymph nodes from the aortic area If none of the lymph nodes are cancerous, radiation therapy is still possible are selected if the tumor is large, if the tumor has grown into the bloodstream or lymph nodes, or if the tumor has invaded surrounding connective tissue affecting organs such as the uterus, bladder, or vagina. If the cancer has spread to tissues next to the uterus or to any lymph nodes, radiation therapy (EBRT) is usually recommended. Your doctor may also advise other methods of treatment after a combination of chemotherapy and radiation. Using both radiation therapy and external beam radiation therapy may be an option if a woman is not healthy enough for surgery or if she decides she does not want surgery Chemotherapy may be given with radiation. radiation (concurrent chemotherapy). 2.5 Stages IB2 and IIA2 Treatment options:
Chemotherapy: This is usually the standard treatment. Chemotherapy may be using cisplatin or cisplatin in combination with fluorouracil. Radiation therapy includes both external-beam and para-radiotherapy. Radical hysterectomy with pelvic lymph node dissection and aortic lymph node sampling: If cancer cells are found in the removed lymph nodes, or in the edges of the removed tissue, there is Treatment can be continued with radiation therapy, often in combination with chemotherapy. 2.6 Stages IIB, III and IVA Treatment options:
Chemotherapy: Chemotherapy may be cisplatin or cisplatin plus fluorouracil. Radiation therapy includes both external-beam and para-radiotherapy. 2.7 Stage IVB At this stage, cancer has spread beyond the pelvis to other areas of the body. Stage IVB cervical cancer is not usually considered curable. Treatment options include radiation therapy and/or chemotherapy to try to slow the growth of the cancer or help relieve symptoms. Most standard chemotherapy regimens include one drug cisplatin or carboplatin along with another drug such as paclitaxel (Taxol), gemcitabine (Gemzar), or topotecan. The drug bevacizumab (Avastin) can be added to chemotherapy or immunotherapy alone with pembrolizumab (Keytruda®) also may be an option.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.