This is an automatically translated article.
The article was written by MSc Vu Huu Thang - Emergency Medicine Doctor, Emergency Department - Vinmec Ha Long International Hospital.Hellp syndrome is an obstetric pathology characterized by hemolytic anemia, elevated liver enzymes, and thrombocytopenia. Occurs in the second half of pregnancy. The morbidity rate is 2% - 12%, the maternal mortality rate is 35%. Because of the potential for maternal and fetal death, HELLP syndrome is truly an emergency requiring urgent diagnosis and management in the obstetrics and intensive care unit. In Vietnam, there are no accurate data on the incidence of HELLP syndrome.
1. Causes of Hellp Syndrome
The cause is not clear, there are many controversies. However, the majority of authors agree on the nature of HELLP as a special clinical form of preeclampsia.
2. Hellp Symptoms
2.1 Clinical The majority of HELLP syndrome occurs against a background of toxemia of pregnancy (pre-eclampsia or eclampsia).
+ Phew.
+ Increased blood pressure .
+ Pregnancy > 20 weeks.
+ HELLP syndrome occurs in about 4 - 12% of patients with pre-eclampsia, about 30% of cases of HELLP appear in the first weeks postpartum.

Mẹ bầu có thể gặp tình trạng phù khi mắc hội chứng HELLP
Manifestations:
+ Feeling uncomfortable (90%)
+ Epigastric pain (65%)
+ Headache (31%): severe pain, blurred vision, excitability, increased reflexes
+ Sad vomiting and vomiting
+ Edema, hypertension, jaundice, subcutaneous hemorrhage
+ Eclampsia: on the background of preeclampsia, convulsions appear, showing damage to the central nervous system
2.2 Subclinical Hemolysis: occurs in the blood capillaries, due to the transport of red blood cells in the lumen of the blood capillaries is damaged. Signs of hemolysis include: + Broken red blood cells, deformed red blood cells on the slide.
+ Blood bilirubin increased.
+ Haptoglobin increased.
+ LDH increases.
Increased GOT, GPT: caused by ischemia in the liver, can lead to liver infarction, these lesions explain the symptoms of epigastric pain, vomiting, nausea or right upper quadrant pain, jaundice. Thrombocytopenia: due to microvascular damage mainly endovascular damage and vasospasm. The consequence of serotonin and thromboxane A2 is increased intravascular platelet aggregation.

Xét nghiệm máu giúp bác sĩ chẩn đoán hội chứng Hellp
3. Diagnosis of Hellp's syndrome
3.1 Definitive diagnosis On the background of a patient with gestational toxicity (pre-eclampsia, eclampsia), a triad appears:
Hemolysis: + Peripheral blood abnormalities: erythrocyte fragmentation, erythrocyte abnormalities form.
+ Indirect bilirubin > 1.2 mg/dl.
+ LDH > 600 U/L
Elevated liver enzymes: GOT or GPT > 70 U/L Thrombocytopenia: platelet count < 100,000/mm3 3.2 Differential diagnosis Thrombocytopenic purpura. Disseminated intravascular coagulation. Antiphospholipid antibody syndrome. Malignant hypertension. Hemolytic anemia with high uremia. Viral hepatitis. Bile duct infection. Toxic hepatitis. Acute fatty liver disease in pregnant women. Table of differential diagnosis of HELLP syndrome
4. Classification of HELLP . syndrome
2 ways to classify:
According to MEMPHIS: + Partial HELLP syndrome (with 1 or 2 abnormal signs).
+ Full HELLP syndrome: there are many complications for the mother and the pregnancy should be terminated.
Based on platelet count: + Grade I: < 50,000 mm3
+ Grade II: 50,000 – 100,000 mm3
+ Grade III: 100,000 – 150,000 mm3
(The level of power depends on the platelet count)
5. Complications of HELLP . syndrome
Disseminated intravascular coagulation (DIC). Young vegetables. CKD . Pulmonary edema . Hematoma under the liver capsule. Bleeding complications.
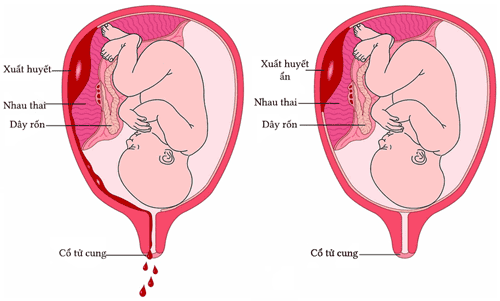
Biến chứng hội chứng HELLP có thể gây rau bong non
6. Treatment of Hellp's syndrome
6.1 Treatment of mother Low blood pressure:
+ Should control blood pressure < 150/90 mmHg, it is best to lower the blood pressure number to about 10-15% of the initial number in the first few hours.
+ Should use intravenous antihypertensive drugs with quick action, short, easy to adjust, oral drugs are gradually replaced intravenous infusion.
+ Preferred drug: Loxen (Nicardipine) dose 1 - 5 mg/hour, gradually increasing oral medication Nifedipine, labetalol.
+ Prevention of convulsions: Magnesium sulphate intravenous bolus dose of 2 - 4 g, then maintain intravenous infusion 1 - 2 g/hour (with caution in renal failure).
Use of blood products:
+ Blood transfusion should only start when Hct < 25%, especially when cesarean section.
+ Platelet transfusion: the purpose of preventing bleeding when surgical intervention or delivery is required (platelet transfusion when platelets are < 20,000/ml).
Fluids :
Based on monitoring of CVP and urine volume.
Một số trường hợp, mẹ bầu được truyền máu khi can thiệp phẫu thuật
6.2 Assessment of fetal status The timing of pregnancy termination depends on the mother's medical condition, response to treatment, fetal health status and fetal maturity.
Prognosis:
The maternal mortality rate is about 10%, the child mortality rate is from 10% to 60% depending on the mother's medical condition. 20% - 30% will have HELLP syndrome in the next pregnancy and 40% will have preeclampsia in subsequent pregnancies. Vinmec International General Hospital offers a Package Maternity Care Program for pregnant women right from the first months of pregnancy with a full range of antenatal check-ups, periodical 3D and 4D ultrasounds and other routine tests to ensure the mother is healthy and the fetus is developing comprehensively. Pregnant women will no longer be alone when entering labor because having a loved one to help them during childbirth always brings peace of mind and happiness.
References:
Vu Van Dinh (2000): “Preeclampsia and eclampsia”. Emergency Manual, Medical Publishing House, pp.529-532.
Abildgaard U., Heimdal K. (2013), “Pathogenesis of the syndrome of hemolysis, elevated liver enzymes, and low platelet count (HELLP): a review”.
Eur J Obstet Gynecol Reprod Biol. 166, Pp.117.
Alan D., Lauren N. (2013), “HELLP syndrome”, Current therapy in Obstetrics and Gymecology 11, Pp. 288 – 293.
Benedetto C., Marozio L., Tancredi A. et al. (2011), “Biochemistry of HELLP syndrome”, Adv Clin Chem, Pp. 53-85.
Burwick R.M., Feinberg B.B. (2013), “Eculizumab for the treatment of preeclampsia/HELLP syndrome”, Placenta. 34, Pp. 201.