This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II Le Thanh Cam - Department of Pediatrics - Neonatology - Vinmec Danang International General Hospital.Cleft palate accounts for the highest proportion of general malformations of the body (10%), in which cleft palate is a very rare complex craniofacial abnormality that causes severe psychological and aesthetic effects. aesthetics and function of the patient.
1.Overview
Birth defects of maxillofacial, mainly cleft palate, have the rate of 1/1000 newborns. In the maxillofacial department, the number of patients who come to treat cleft lip and palate malformation accounts for about 20%. Among them, Tessier No. 4 is an anomaly in the ophthalmic cleft which is very rare (1.43 - 4.85/100,000 children).
The pathological feature is the cleft from the lower eyelid margin to the upper lip (between the nucleus pulposus and the corners of the mouth). Accompanying these are conjunctival malformations, eyes are not closed, causing the eyeball to be unprotected, the risk of inflammation, corneal dryness, conjunctiva, eyeball atrophy or no eyeball, jaw bone defect, severely affect the structure and function of the patient's face.
2. Pathogenesis

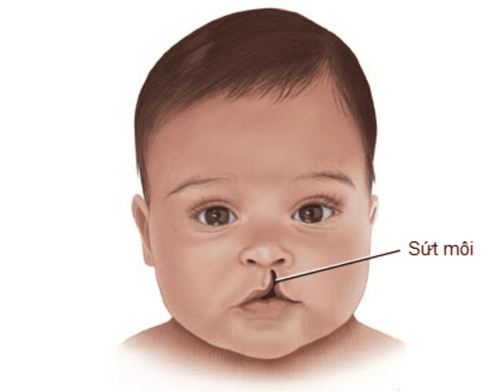
Khe hở môi vòm miệng ở trẻ
The bud theory of Rhatke (1832), Dursy (1869) and His (1888) suggested that the process of forming the lips and palate is due to the fused facial buds. If for some reason (intrinsic or extrinsic) affects the development and attachment of the facial bud, it will lead to corresponding birth defects of the maxilla.
From the above theory, we can have the following types of clefts:
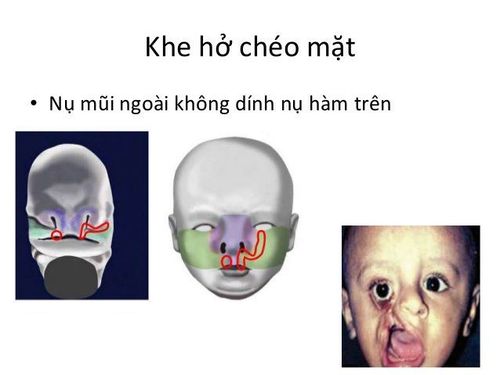
Cleft lip between the upper jaw: due to 2 buds not sticking together. Cleft lip on the upper jaw: when the bud of the upper jaw is not attached to the inner nasal bud. Lower lip cleft: when 2 lower jaw buds do not stick together. Horizontal cleft: when the upper bud is not attached to the lower jaw. Cross-facial cleft: when the outer nasal bud does not adhere to the upper jaw bud. Soft palate cleft: 2 posterior transverse buds are non-adherent. Hard palate cleft: 2 anterior transverse buds not adherent. Note:
It is possible to have a cleft lip without a cleft palate, but the reverse is not possible. It is possible to have a soft palate without a hard palate, but the reverse is not possible.
3.Cause
There are 2 types of causes of congenital malformations of the maxillofacial (including Tessier's cleft palate no. 4):
Exogenous causes
Physical factors: thermal, mechanical, radioactive. Chemical factors: fetal hypoxia, malnutrition, endocrine disorders, pregnancy toxicity. Biological factors: Infection with viruses during pregnancy (influenza), bacteria and toxins, parasites. Neurological factors: (mother panic, stress, depression) Intrinsic cause
Genetic factors. Biological defect of sex cells. Effects of age at birth and race (eg: mothers over 40 years old) Usually external causes account for 70% of cases of craniofacial malformations (including unknown factors), and 30% are due to other factors. intrinsic factor.

Thai thiếu oxy là nguyên nhân nội tại gây ra dị tật bẩm sinh hàm mặt
4.Classification of maxillofacial congenital anomalies
There are 4 major clefts in maxillofacial malformations :
4.1. Cleft lip and jaw Cleft lip malformation is characterized by a cleft in the red lips and skin, without damage to the maxillary bone. Classified by degrees:
Mild (grade 1⁄3): red lips with upward defect. Moderate (grade 2⁄3): Cleft involves the red lip and half of the skin of the upper lip. Severe (grade 3/3): the entire upper lip is divided from the red lip to the nasal cavity (total cleft lip), accompanied by deformity of the alar. Cleft palate malformation is characterized by the presence of bone in front of the incisors (anterior palatal foramen) according to the following levels:
Mild: there is a slight dent in the maxillary lateral incisor area. Moderate: there is a gap in the alveolar bone. Severe: there is a bony cleft to the incisor foramen. 4.2. Cleft hard palate and soft palate Soft palate cleft (nasopharynx):
Cleft uvula. Cleft of the uvula and the cleft of the middle third of the soft palate. Total soft palate cleft. Hard palate cleft:
Cleft to posterior 1/3. Clearance to the middle 1/3. Cleft palate to the incisor foramen area.
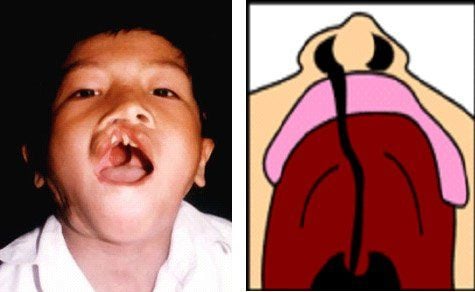
Khe hở vòm miệng
4.3. Cleft palate and lip coordination A defect that combines the cleft lip and palate together, often more complex and difficult to treat.
4.4. Other special clefts Including upper-middle cleft, lower lip cleft, crossfacial cleft, transverse cleft. These types of malformations are rarely seen on the face and occur very rarely.
To accurately diagnose the type of cleft palate, it is necessary to analyze and evaluate the following factors:
Side of cleft: One side (right or left) or both sides. Degree of cleft more or less: Not total, total, or grade 1, grade 2, grade 3 Preliminary assessment of cause of malformation: eg, total cleft lip may be caused by influenza virus; Bilateral degree 1 cleft lip can be caused by genetic factors...
5.Treatment measures
To treat congenital malformations of the face and face, it is necessary to closely coordinate with many specialties (called complex treatment). This complex treatment lasts from birth to adulthood (20-25 years). In which, surgical treatment can be intervened from a few months old depending on the deformity, location, and health status of the patient.
Currently, surgical methods to treat cleft palate are often not clearly described, making thorough treatment difficult, patients often have to have many surgeries to repair. Normal surgery is already complicated, it is more difficult to correct the wrong surgery, as well as affect the patient's psychological and economic well-being. Therefore, children with complex congenital malformations should be brought to the clinic for examination, diagnosis and treatment by doctors who are experienced and skilled in the treatment of clefts of the face.
Resuscitation and postoperative care also play an important role in the outcome of surgery and should be performed in large hospitals and medical centers with highly qualified medical staff.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.