This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Nguyen Thi Mai - Radiologist - Diagnostic Imaging Department - Vinmec Phu Quoc International General Hospital.More than 2000 patients die from thyroid cancer each year. Although, thyroid cancer is often treatable and curable with surgery. Therefore, the application of comprehensive measures to diagnose thyroid cancer early will greatly help the treatment of this disease.
Epidemiology
Thyroid cancer (TG) accounts for about 1-2% of cancers of the general organs, but accounts for up to 90% of cancers of the endocrine glands. Annually with 45,000 new cases and 1,700 deaths recorded in the US. The risk of the disease increases with age. In Vietnam, in Hanoi, the prevalence is 1.9/100,000 population, male/female is 1/2,6. The etiology and pathogenesis of the disease are unclear.Women have more thyroid cancer than men, the female/male ratio is 3:1.
Comprehensive measures to diagnose thyroid cancer
Currently, there are many methods used to diagnose thyroid cancer, including imaging methods. Imaging helps to determine the presence or absence of lesions, assessing the stage of the cancer contributes to the treatment plan for each stage. Besides, the diagnostic methods used are often based on:
Hiện nay có nhiều phương pháp được sử dụng để chẩn đoán ung thư tuyến giáp
1. Thyroid ultrasound
Provides useful information on thyroid tumor size and location, identifies cystic lesions, detects palpable nodules or abnormal cervical lymph nodes, especially notes suggestive features. Note malignancy (eg, microcalcifications in the nucleus, irregular margins, angiogenesis within the mass). Simple cystic lesions, which can be found in about 10% of patients with palpable thyroid nodules, with a malignancy rate <1% have been reported. Ultrasonography can be difficult to reliably distinguish between benign and malignant lesions, especially with mixed lesions with solid and cystic components or purely solid. TI-RADS Classification (2017)2. Thyroid scan
It can be performed in non-pregnant patients who present with abnormal thyroid lesions while TSH levels are low, in order to identify the “hot” cause of increased thyroid hormone secretion. A "cold" nodule is detected in about 90% of patients with palpable thyroid nodules, both benign and malignant, however, only 10% of "cold" nodules are identified as thyroid cancer. Therefore, thyroid scintigraphy for all thyroid nodules is not indicated, except when TSH levels are low.3. Thyroid Biopsy
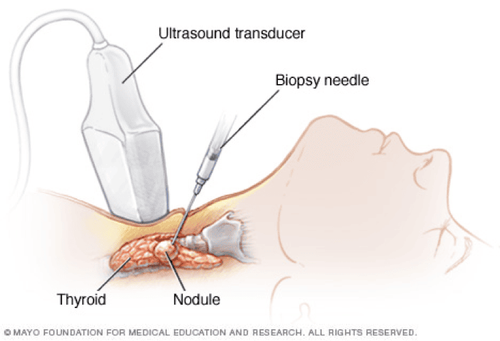
Fine needle aspiration: an extremely valuable test in diagnosing the nature of thyroid nodules, in order to limit unnecessary surgical indications. Many practice guidelines recommend aspiration cytology as a first-line test for thyroid nodules. In cases where the tumor is not clinically palpable, ultrasound-guided aspiration cytology should be indicated if there are imaging findings suspicious of malignancy Open biopsy: ordered with Suspected thyroid lesion, not elucidated with fine-needle aspiration test.
Chọc hút bằng kim vô trùng giúp bác sĩ chẩn đoán ung thư tuyến giáp
4. Quantification of serum calcitonin
Intended for patients with a family history of myeloid carcinoma or other forms of the MEN-2 syndrome. Normal initial results will require a calcitonin stimulation test using pentagastrin or intravenous calcium. Patients with elevated calcitonin levels require careful investigation (even exploratory neck surgery) even though physical examination or ultrasonography are unremarkable.5. Some other tests
Computed tomography of the head and neck is indicated in the clinical picture of a large invasive tumor (vocal paralysis, airway compression), cervical lymph node metastasis to evaluate the extent and stage of the tumor. Chest x-ray, abdominal ultrasonography, and alkaline phosphatase should be routinely indicated in the evaluation of systemic metastases. Bone scintigraphy will be indicated next in case of elevated serum ALP. - Computed tomography of the chest and abdomen when the patient has signs suggestive or undifferentiated breast cancer.6. Histopathology
Histopathologically more malignant forms tend to be more common in older patients.6.1 Papillary carcinoma accounts for about 80% of malignancies in adults, most often in younger patients. - In terms of histological structure, tumor cells can be arranged in papillary or follicular structure. The diagnosis of papillary carcinoma is based on the characteristics of the nucleus, not on the presence or absence of cystic structures. The psammoma (also called the “sand” body – spherical calcium deposition nodules) can be seen in about 40% of cases. Cervical lymph node metastases may occur in about 50% of patients with papillary carcinoma. Distant metastases to lungs, bones, skin and organs appear late 6.2. Follicular cancer The incidence is approximately 10% of breast cancer, the peak of incidence is between the ages of 40 and 50. - Follicular carcinoma tends to invade blood vessels and metastasize by blood to organs, especially is bone. Lymph node metastases are relatively rarer than papillary ones. 6.3. Anaplastic cancers account for 1-2% of breast cancers. Usually occurs in patients over 60 years of age. Aplastic breast cancer is very malignant, rapidly invades surrounding tissues and metastasizes to other organs. 6.4. Medullary cancer accounts for 5-10% of cervical cancers, secreting calcitonin and CEA. In addition, ACTH, histamine, and an unidentified substance may also be secreted by the tumor cells themselves. Metastatic lesions are common in cervical and mediastinal lymph nodes, possibly with calcification. Distant metastases in organs appear late 6.5. Hurthle cell carcinoma is considered a variant of follicular carcinoma, with a relatively more malignant natural course.

Di căn hạch cổ có thể gặp ở khoảng 50% bệnh nhân UTTG thể nhú
Thyroid cancer is becoming more and more common and tends to increase. Although the cure rate is quite high, it is not possible to underestimate thyroid cancer. Regular periodic health check-ups to detect thyroid abnormalities early so that appropriate treatment can be given. It can be ultrasound, X-ray, computed tomography, blood tests or endocrine tests... to make an accurate diagnosis of thyroid cancer.
Vinmec International General Hospital is equipped with advanced modern equipment and a team of leading experts with high expertise. The hospital now has an effective screening and screening package for thyroid diseases, helping to check thyroid function, screening & early detection of common thyroid diseases such as simple goiter, hyperthyroidism, hypothyroidism, thyroiditis, thyroid nodules, thyroid cancer, ... so that appropriate and timely treatment measures can be taken.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.