This is an automatically translated article.
The article was professionally consulted with Doctor Pham Thi Mai Nhung - Obstetrician and Gynecologist - Department of Obstetrics and Gynecology - Vinmec International Hospital Da Nang.Polycystic ovary syndrome (PCOS) is a common endocrine disorder in women. This is a syndrome characterized by polycystic ovaries on ultrasound and hyperandrogenism manifest either subclinically (hypergonadotropic hormone) or clinically (menstrual irregularity, obesity, hirsutism) hair, acne). To diagnose polycystic ovary syndrome, it is necessary to conduct basic tests.
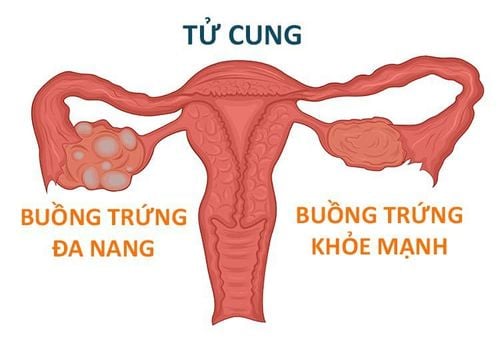
1. What is polycystic ovary?
In polycystic ovary disease characterized by signs of multiple cysts in the ovaries when observed on ultrasound, accompanied by symptoms of virilization (hirsutism, acne, baldness) and menstrual disorders. .Patients with PCOS have resistance to insulin (an important hormone in the body's blood sugar regulation). The hypothesis for the pathogenesis of polycystic ovary syndrome is still unknown, but PCOS has been found to be strongly related to hyperinsulinism. High blood insulin levels are thought to be associated with hyperandrogenism due to increased androgen production in the ovaries and decreased synthesis of sex hormone-binding proteins, which affects ovarian function.
It has been found that in people with PCOS, the levels of EGF and TGF are increased, inhibiting the development of ovarian follicles as well as inhibiting the aromatic process of converting Androgen to Estrogen of granulosa cells. Besides, IGF-1 secreted from the cortex cells increases the synthesis of Androgen. Finally, the concentration of Androgen in the follicular fluid increases, causing the ovarian follicles to degenerate. In addition, when the aromaticization of estrogen synthesis is inhibited, estrogen levels are not high enough to give negative feedback to the hypothalamic axis, uninhibited LH continues to rise. All of the above factors contribute to the predominance of azoospermia and accelerated follicular degeneration.
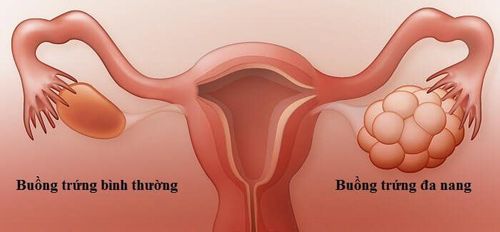
2. Manifestations of polycystic ovaries

Buồng trứng đa nang còn có tình trạng kháng insulin
Polycystic ovaries also have insulin resistance. This is a condition in which some organs respond less than normal to the same amount of insulin, causing hyperinsulinemia and type II diabetes. Insulin resistance is often accompanied by a variety of other metabolic disorders, leading to high blood pressure, dyslipidemia such as: increased triglycerides, increased LDL, decreased HDL, increased waist circumference.
Hyperandrogenism in women with PCOS leads to symptoms such as: Hirsutism; develops in places like the cheeks, chin, neck in the middle of the chest and below the navel, acne, baldness, hair loss.
3. Diagnostic criteria for polycystic ovary
Diagnosis is confirmed when 2 of the following 3 criteria are present and other causes are excluded.Criterion 1: Ovulation disorder or anovulation. Manifestations of menstrual disorders:
Menstrual irregularities: Menstrual cycles over 35 days or menses <8 times/year. Amenorrhea: Over 6 months without amenorrhea. Criterion 2: Hyperandrogen (clinical and subclinical)
Clinical:
Symptoms of hirsutism, acne, baldness, keratosis. Abdominal obesity, BMI (Body Mass Index) > 25, waist/hip ratio (waist/hip ratio): > 0.85. Subclinical:
Increase in Total Testosterone, increase in Free Testosterone (T > 2.5 nmol/ml) Increase in LH > 10mUI/ml, LH/FSH ratio >2 Decrease in SHBG (Sex Hormone Binding Globulin), decrease in IGFBP- 1 (Insulin like Growth Factor Binding Protein). Elevated free estradiol Criterion 3: Polycystic ovary image on ultrasound (survey on day 2-5 of menstrual cycle or day 3 of artificial cycle).
Number of follicles: over 12 follicles size from 2-9 mm. Ovarian volume greater than 10 cm3. (Regardless of cyst distribution or ovarian tissue density.)
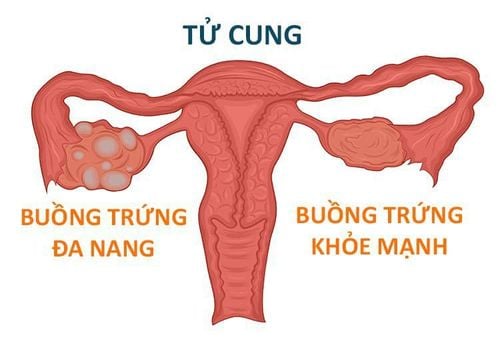
Buồng trứng đa nang còn có tình trạng kháng insulin
4. Diagnostic test for polycystic ovary syndrome
4.1 Pre-diagnostic screening tests for polycystic ovary syndrome Certain endocrine disorders with hyperandrogenism similar to polycystic ovary syndrome need to be ruled out before diagnosing polycystic ovary syndrome. .Late congenital adrenal hyperplasia due to 21-hydroxylase deficiency can be ruled out by measuring serum 17-hydroxyprogesterone levels after a cosyntropin stimulation test. 17-hydroxyprogesterone levels below 1000 ng/dL measured 60 minutes after cosyntropin stimulation may help rule out late congenital adrenal hyperplasia.
Women with PCOS should be screened for Cushing's syndrome or acromegaly when there is clinical suspicion for these conditions. Cushing's syndrome can be ruled out by examining a 24-hour urine sample for free cortisol and creatinine. Urinary cortisol levels 4 times the upper limit of normal are diagnostic for Cushing's syndrome. A dexamethasone suppression test is also useful to screen for Cushing's syndrome.
Serum insulin-like growth factor (IGF) 1 should be checked to rule out acromegaly. Serum IGF-1 is a sensitive and specific marker of growth hormone (GH) excess.
A small percentage of patients with PCOS have elevated prolactin levels (usually > 25 mg/dL). Hyperprolactinemia can be ruled out by testing fasting serum prolactin levels.
Phụ nữ bị PCOS nên được kiểm tra hội chứng Cushing
In which the free testosterone index (FTI) is recommended to be used to diagnose hyperandrogenism. Formula to calculate FTI:
FTI=Total Testosterone/SHBG x100.(SHBG: sex hormone-binding globulin).
Androstenedione levels are also increased in women with PCOS. This is an androgen precursor, derived 60% from the ovaries and 40% from the adrenal glands.
Patients with androgen-secreting ovarian tumors or adrenal tumors may present with hirsutism, amenorrhea, and signs of virilization. In these cases, quantification of DHEA-S may provide partial differential diagnosis. DHEA-S is of adrenal origin, and thus elevation of DHEA-S would be suggestive of adrenal origin.
4.2.2. Quantification of FSH and LH Follicle-Stimulating Hormone (FSH) secreted by the anterior pituitary gland. During the follicular phase of the menstrual cycle, FSH initiates the production of estradiol by Graff's follicles, which then work in tandem to help further ovarian follicles grow. Sudden increases in FSH and luteinizing hormone (LH) levels midway through the menstrual cycle trigger ovulation.
During the luteal phase, FSH stimulates the production of progesterone and this hormone, along with estradiol, facilitates the ovarian response to LH.
Follicle-stimulating hormone (FSH) levels should be checked to rule out primary ovarian failure. In patients with PCOS, FSH levels are in the normal or low range. Increased levels of luteinizing hormone (LH) depend on reproductive stage, sex, and age. The LH-FSH ratio is usually greater than 3.
Stimulation test with a long-acting gonadotropin agonist (GnRH) causes a characteristic increase in ovary-derived 17-hydroxyprogesterone after 24 h. Results reflect excessive 17-hydroxylase activity.

Kiểm tra nồng độ hormone kích thích nang trứng (FSH) để loại trừ suy buồng trứng nguyên phát
Persistent primary hypothyroidism may be associated with markedly elevated levels of thyroid-stimulating hormone (TSH). The hormone TSH contracts the same alpha subunit as FSH and LH, so elevated levels of the alpha subunit of TSH can cross-react with the FSH and LH receptors in the breast tissue, leading to premature thelarche and, in the tissue. ovaries, resulting in a PCOS-like picture. Physical findings of van Wyk-Grumbach syndrome (adolescent hypothyroidism, precocious puberty and ovarian enlargement) treated with thyroxine add-on therapy.
4.2.4. Glucose, Insulin, and Lipids Because the rates of impaired glucose tolerance and type 2 diabetes are so high in women with polycystic ovary syndrome (PCOS) who have a greater body mass index (BMI). 30 kg/m2, with a family history of type 2 diabetes, or older than 40 years, a 75 g oral glucose tolerance test (OGTT) should be performed. A 2-hour post-load glucose value below 140 mg/dL indicates normal glucose tolerance; a value of 140-199 mg/dL indicates impaired glucose tolerance; and a value of 200 mg/dL or higher indicates diabetes mellitus. Women diagnosed with PCOS should be screened for gestational diabetes before 20 weeks of gestation. Some women with PCOS often have insulin resistance and dyslipidemia (cholesterol > 200 mg/dL; LDL > 160 mg/dL). Therefore, quantitative blood glucose and lipid tests are essential to monitor treatment for patients with PCOS.
4.3. Imaging tests 4.3.1. Ultrasound In the past, polycystic ovary syndrome was diagnosed by laparotomy and direct visualization of the ovaries. Since the development of ultrasound, it has been routinely indicated in the diagnosis of PCOS because it is noninvasive, painless, simple, and relatively inexpensive.
Ultrasound counts secondary follicles, measures ovarian volume. Ultrasound can be transabdominal or vaginal. Transabdominal ultrasound, the patient needs to drink a lot of water, has the advantage of being able to generalize the organs in the abdomen, including the uterus and ovaries. However, transabdominal ultrasound limits visualization of the ovaries, so transvaginal ultrasonography is usually performed if there are no contraindications.
4.3.2. CT-scan and MRI In certain cases where a tumor is suspected, computed tomography (CT) or magnetic resonance imaging (MRI) to examine the adrenal glands and ovaries helps to differentiate PCOS from certain conditions. other. MRI is a good method for imaging the ovaries and is a useful ultrasound substitute in very obese women, in whom the ovaries may not be seen with ultrasound, and in patients in whom ultrasonography is not possible. Vaginal sounds are not suitable, such as adolescent girls.
In order to help customers detect and treat other gynecological diseases early, Vinmec International Hospital has a basic gynecological examination and screening package, helping customers detect early inflammatory diseases Easy, inexpensive treatment. Screening detects gynecological cancer (cervical cancer) early even when there are no symptoms.
Basic gynecological examination and screening package for female customers, has no age limit and may have the following symptoms:
Abnormal vaginal bleeding Having menstrual problems: irregular menstrual cycle, irregular menstrual cycle Irregular vaginal discharge (smell, different color) Vaginal pain and itching Female clients have several risk factors such as poor personal hygiene, Unsafe sex, abortion,... Female customers have other symptoms such as: Abnormal vaginal discharge, itching, pain in the private area, abnormal vaginal bleeding.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References: webmd.com, nhs.uk, mayoclinic.org